 |
Bios Dr. Tseng is a vitreoretinal surgery fellow at the University of Washington in Seattle where Dr. Fortenbach is an assistant professor of ophthalmology. DISCLOSURES: The authors have no relevant relationships to disclose. |
A 63-year-old man was referred for acute vision loss in the left eye upon awakening following a myelogram. His medical history was notable for bilateral subdural hematomas secondary to intracranial hypotension caused by a cerebrospinal fluid–venous fistula, with concern for a persistent CSF leak prompting the procedure. On further questioning, the patient reported the new onset of several large central red blotches in his left eye, which had not been present prior to the myelogram.
Examination findings
On presentation, best-corrected visual acuity was 20/20 in the right eye and counting fingers at 2 feet in the left eye. Intraocular pressures and pupillary responses were normal. Anterior segment examination was unremarkable in both eyes. Dilated fundus examination revealed a normal right eye, while the left eye demonstrated a large vitreous hemorrhage centered on the posterior pole with scattered foci of midperipheral preretinal hemorrhages.
Imaging and workup
The referring service requested a computed tomography scan of the head in light of his acute visual changes, which redemonstrated bilateral subdural fluid collections consistent with subdural hematomasfrom his initial study. There was no evidence of acute infarct or new intraparenchymal hemorrhage. Our service also obtained
Optos pseudocolor fundus photography and an OCT of the macula during his initial outpatient follow-up, demonstrating a dense central vitreous hemorrhage in his left eye (Figures 1 and 2A).
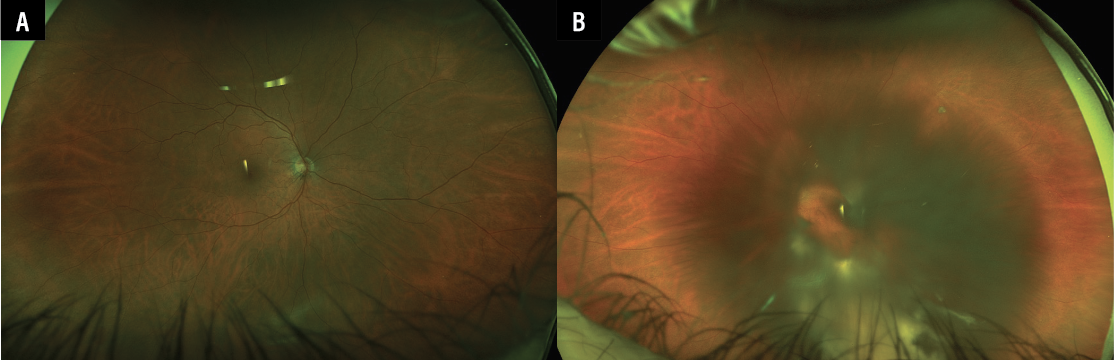 |
| Figure 1. Optos pseudocolor fundus photographs of (A) the unaffected right eye and (B) the left eye, demonstrating a dense, largely dehemoglobinized central vitreous hemorrhage. |
Diagnosis and management
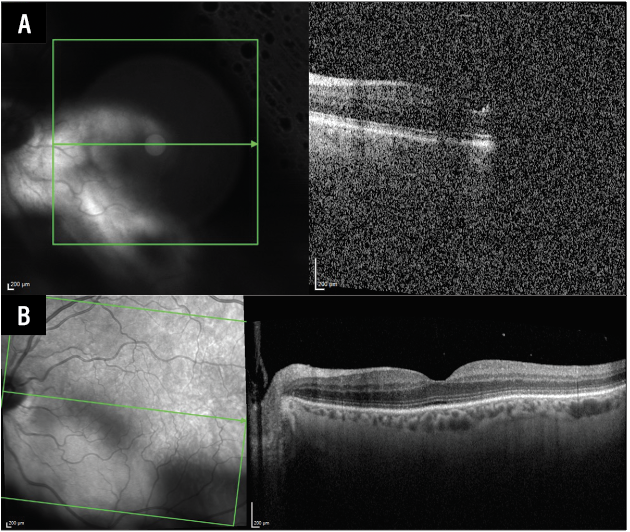
We diagnosed the patient with Terson syndrome, given the presence of the vitreous hemorrhage and preretinal hemorrhages, likely resulting from a transient elevation in intracranial pressure during his myelogram. Following several months of persistent central hemorrhage, he was offered surgery to assist with restoring his vision, but he declined. He was therefore clinically followed over the subsequent 18 months. Over that time, there was a gradual improvement in his vitreous hemorrhage and visual acuity. At his most recent follow-up, BCVA was 20/20 in his right eye and 20/25 in his left eye. There was minimal residual dehemoglobinized vitreous hemorrhage in the left eye, which had cleared from the visual axis, as demonstrated on optical coherence tomography imaging (Figure 2B).
 |
|
Figure 2. Optical coherence tomography of the left eye at the time of presentation demonstrating significant media opacity secondary to vitreous hemorrhage (A), and marked improvement of media opacity at 18-month follow-up (B). |
Discussion
Terson syndrome refers to the presence of intraocular hemorrhage in patients with intracranial hemorrhage or other conditions that cause an acute rise in intracranial pressure.1 It’s most commonly associated with aneurysmal subarachnoid hemorrhage, with reported incidence ranging from 8 to 44 percent.2 Despite this, TS is likely underdiagnosed, as affected patients often have neurological deficits that limit their ability to report visual symptoms, resulting in delayed ophthalmologic assessment. Although well described in the setting of intracranial hemorrhage, TS has only rarely been reported following procedures such as myelography, pneumoencephalography or ventriculostomy.3,4
The exact pathophysiology of TS remains incompletely understood, but the leading hypothesis involves a rapid increase in intracranial pressure that’s transmitted along the optic nerve sheath.5 This results in compression of the central retinal vein and impaired venous outflow, ultimately leading to rupture of fragile retinal capillaries. Alternative proposed mechanisms include direct transmission of blood from the intracranial to intraocular compartments through either the lamina cribrosa or perivascular (Virchow-Robin) spaces within the optic nerve.5
The presence of TS is associated with a poor neurological prognosis, as well as increased morbidity and mortality.6 From an ophthalmologic perspective, however, the natural course of TS is generally favorable. While many cases see spontaneous resorption of the hemorrhage, surgical intervention can accelerate visual recovery. Surgery is typically indicated in cases of dense bilateral vitreous hemorrhage, when visual recovery is delayed for more than four to six months, or to prevent amblyopia in children.1
The timing of surgery remains a topic of debate. There’s no consensus on the optimal timing of vitrectomy, as some studies report no significant difference in visual outcomes between patients undergoing surgery within three months of developing vitreous hemorrhage and those treated later.7 In contrast, other studies suggest that earlier intervention is associated with improved visual outcomes and a lower risk of intraoperative and postoperative complications, including retinal detachment, optic disc atrophy and maculopathy.8,9 In addition to vitreous hemorrhage, epiretinal membranes and macular holes—whether occurring spontaneously or following surgery—are also recognized sequelae of TS, which may necessitate additional intervention, such as repeat vitrectomy with membrane peeling.5,10
Ultimately, management of TS requires a multidisciplinary approach between ophthalmology, neurology and neurosurgery. Increased awareness among clinicians is essential to ensure timely diagnosis and intervention, particularly as visual impairment may significantly impact quality of life in patients recovering from neurologic injury. RS
REFERENCES
1. Stevanovic M, Eliott D. Terson syndrome: A review of the literature.
Int Ophthalmol Clin 2024;64:2:89-106.
2. Lee GI, Choi KS, Han MH, Byoun HS, Yi HJ, Lee BR. Practical incidence and risk factors of Terson’s syndrome: A retrospective analysis in 322 consecutive patients with aneurysmal subarachnoid hemorrhage. Journal of Cerebrovascular and Endovascular Neurosurgery 2015;17:3:203-208.
3. Oberman J, Cohn H, Grand MG. Retinal complications of gas myelography. Archives of Ophthalmology 1979;97:10:1905-1906.
4. Slagsvold JE, Larsen JL. Retinal haemorrhage as a complication of gas encephalography and gas myelography. Prospective study using oxygen gas with a discussion of pathogenetic mechanisms. Journal of Neurology, Neurosurgery, And Psychiatry 1977;40:11:1049-1052.
5. Aboulhosn R, Raju B, Jumah F, et al. Terson’s syndrome, the current concepts and management strategies: A review of literature. Clinical Neurology And Neurosurgery 2021;210:107008.
6. Fountas KN, Kapsalaki EZ, Lee GP, et al. Terson hemorrhage in patients suffering aneurysmal subarachnoid hemorrhage: Predisposing factors and prognostic significance. Journal of Neurosurgery 2008;109:3:439-444.
7. Narayanan R, Taylor SC, Nayaka A, et al. Visual outcomes after vitrectomy for Terson syndrome secondary to traumatic brain injury. Ophthalmology 2017;124:1:118-122.
8. Garweg JG, Koerner F. Outcome indicators for vitrectomy in Terson syndrome. Acta Ophthalmologica 2009;87:2:222-226.
9. Liu X, Yang L, Cai W, Gao L, Li Y. Clinical features and visual prognostic indicators after vitrectomy for Terson syndrome. Eye (London, England) 2020;34:4:650-656.
10. Zhang Y, Lei C, Huang X, Zhang M. Delayed macular hole secondary to Terson syndrome: A case report and literature review. The Journal of International Medical Research 2024;52:3:3000605241233125.



