Take-home points
|
 |
Bio Dr. Brodie is co-founder of Long Bridge Medical (South San Francisco, Calif.) and is an assistant professor of ophthalmology at the University of California San Francisco. DISCLOSURES: Dr. Brodie is an equity holder of Long Bridge Medical and holds patents related to the prosthetic capsular bag. |
If you’re a vitreoretinal surgeon, you’ve likely stood in the operating room, staring at a haptic that won’t cooperate, mentally running through all the intraocular lens gymnastics you can attempt — knowing that none of these options were designed for what you’re about to do. The challenge of IOL fixation in the absence of capsular support is one of the most vexing surgical challenges in our field, and despite years of creative surgical innovation and hundreds of technique papers, the fundamental issue remains: We are repurposing IOLs for a job they were never built to do.
The American Academy of Ophthalmology has published two Ophthalmic Technology Assessments on this topic, spanning 17 years.¹,² Neither identified a superior technique among the many reviewed. Complication rates remain stubbornly high, and we continue to rely on creative workarounds rather than a purpose-designed solution.
The problem that we’ve been living with
Although anterior chamber IOLs remain the only FDA-approved option for eyes without capsular support, there’s well-documented association with corneal decompensation, chronic inflammation and elevated intraocular pressure.1-3 These concerns have led most vitreoretinal surgeons to consider many of their patients poor candidates for ACIOLs, and survey data confirm that only a minority of secondary IOL cases receive an ACIOL today.4
Two surgical approaches dominate in the United States today: sutureless intrascleral fixation, popularized by Dr. Shin Yamane,5 and scleral suturing of IOLs. Both require off-label use of IOLs approved only for in-the-bag placement. The materials, size and design of these lenses are simply not optimized for scleral fixation, and the ad hoc modifications required—flanging, suturing and gluing—make these procedures technically demanding and time-consuming.
The downstream consequences are well-documented. Scleral-sutured IOLs place fixation stress on the suture itself, and late dislocation from suture degradation remains a persistent concern.6,7 Even with Gore-Tex, which has improved breakage rates over polypropylene, recent data show 10 to 39 percent of patients experience at least one complication depending on IOL type.8 Suture tension is another challenge: too loose and the IOL moves; too tight and the haptic optic junction can fracture or suture can erode through tissue—so-called “cheese wiring.”9,10
Sutureless techniques avoid peritomy, but two-point fixation introduces inherent risk of tilt and instability.11,12 The IOL depends entirely on intrascleral compression, and the forces on the haptic-optic junction were never part of the IOL design.¹³ Reports of haptic rotation within the optic (most notably with the CT Lucia) underscore the risk of pushing IOLs beyond their intended purpose.14 In the case of the Carlevale lens, available in Europe but not in the United States, a scleral fixation-specific design has been attempted, but a recent meta-analysis of 608 eyes still showed an average complication rate of 22 percent.15
There’s also an anatomic concern that deserves more attention. Most current fixation techniques route through the pars plicata, a vascular, functionally complex region of the ciliary body, because conventional IOLs lack the diameter and elasticity required for pars plana fixation. This choice is not surgical preference; it’s a limitation imposed by existing lens design options.
Lastly, because these techniques are ad hoc, they lack dedicated reimbursement codes and their complexity prolongs surgical times. Together, these factors make secondary lens cases among the least cost-effective procedures for both surgeons and surgery centers.16
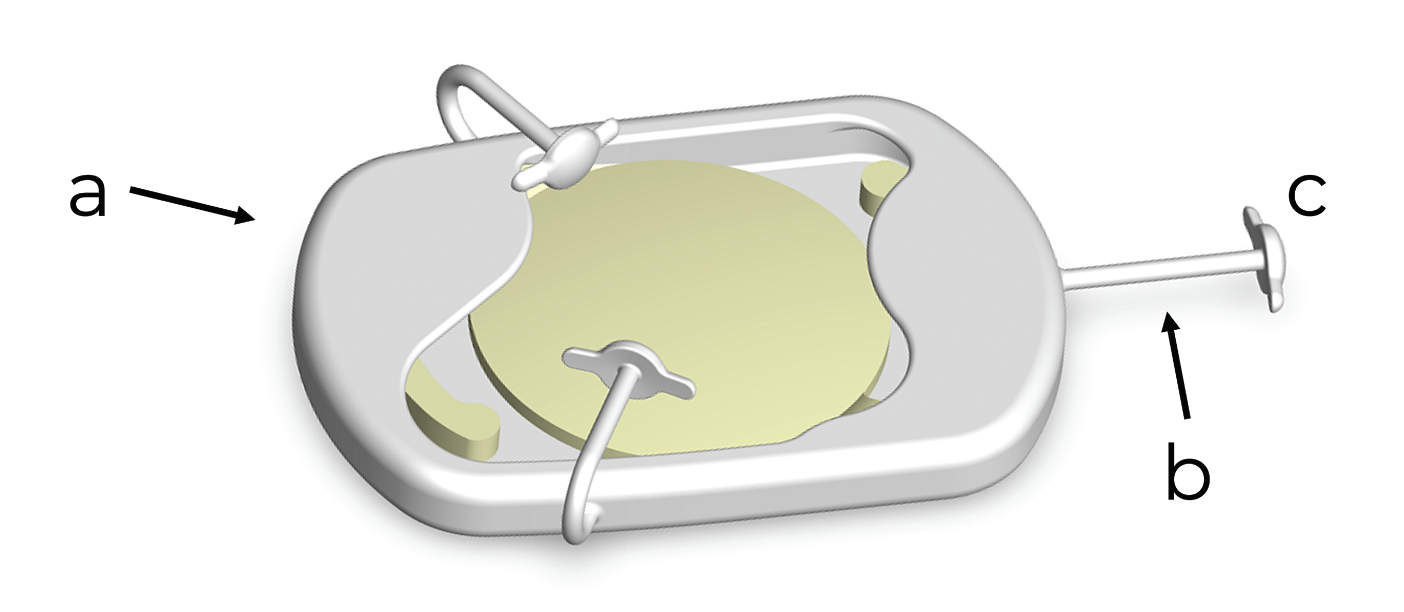 |
| Figure 1. The central housing (a) of the prosthetic capsular bag can accommodate a range of IOLs. It has three fixation arms (b) that end in low-profile footplates (c) that allow sutureless, transscleral fixation through 25- or 27-gauge sclerotomies. |
A device designed for the job
The prosthetic capsular bag was developed to solve these problems from first principles. Intended for patients who are poor candidates for an anterior chamber IOL, the PCB provides a purpose-built platform for safe, reliable posterior chamber fixation in the absence of capsular support.
The device is a flexible silicone elastomer that recapitulates the anatomy and function of the native capsular bag. A central IOL housing was designed to accommodate a wide range of currently used IOLs: single-piece; three-piece; and premium designs (Figure 1a). Three fixation arms, spaced 120 degrees apart (Figure 1b), terminate in low-profile footplates that enable sutureless, transscleral fixation through standard 25- or 27-gauge sclerotomies (Figure 1c). Critically, the silicone elastomer’s elastic properties and functional diameter allow the device to be placed through the pars plana 4 mm posterior to the limbus, avoiding the pars plicata entirely.
PCB insertion employs a standard IOL injector through a corneal incision as small as 2.4 mm (when the IOL is not preloaded), followed by a handshake technique to externalize each footplate through existing vitrectomy cannula sites (For an animation illustrating the loading and insertion, visit https://vimeo.com/longbridgemedical/ani
mation). Three-point fixation provides inherent planar centration, mitigating the tilt risk associated with two-point techniques. And because the PCB separates the fixation problem from the optical problem, surgeons can stock their usual IOL inventory rather than maintaining a separate set of scleral-fixation-specific lenses.
First-in-human results
We conducted a multicenter, prospective, single-arm first-in-human study in Sydney, Australia, enrolling 15 eyes requiring secondary IOL fixation. Indications included dislocated IOLs (n=10), dislocated crystalline lenses (n=1), and aphakia (n=4). Fourteen of 15 subjects completed 12-month follow-up. (For a video of the surgery, visit https://vimeo.com/longbridgemedical/sur
gery)
The safety profile was encouraging. There was one device-related serious adverse event: footplate reinternalization in a patient with Marfan syndrome at postoperative month 8, which was successfully managed by repositioning through a 27-gauge sclerotomy. There were no cases of IOL dislocation from the PCB, no conjunctival erosion over any of the footplates at 12 months, and no evidence of late or chronic inflammation.
The efficacy data were equally compelling. All subjects had improved uncorrected visual acuity, with an average gain of 12 lines on a logMAR chart. Average UCVA at 12 months was 0.36 logMAR (approximately 20/46), and 71 percent of subjects achieved UCVA within two lines of their preoperative best-corrected acuity. Ninety-three percent maintained BCVA within one line of screening. Refractive outcomes were highly predictable: mean spherical equivalent was 0.12 D (SD 0.39 D), with all of the subjects within 1 D of target.
Importantly, the PCB didn’t interfere with subsequent examination of the peripheral retina with the ability for normal indirect ophthalmoscopy and scleral depression.
Regulatory momentum and what’s ahead
The PCB received FDA Breakthrough Device designation in 2023, which was a recognition of its potential to address a significant unmet need in eyes that are poor candidates for an anterior chamber IOL, a population with no FDA-approved alternative to surgically correct aphakia. In March 2026, the FDA approved the investigational device exemption for a U.S. pivotal trial, with anticipated enrollment beginning this summer.
For the retina community, this represents the first realistic pathway to an FDA-approved, purpose-designed device for posterior chamber IOL fixation without capsular support. The platform nature of the PCB, which decouples fixation from optics, and is compatible with existing IOLs, creates a compelling opportunity to transform a surgical category that has remained challenging and essentially unchanged for decades.
We’re hopeful that the prosthetic capsular bag can bring the same degree of standardization, predictability and safety to secondary IOL fixation that the capsular bag itself brought to modern cataract surgery. RS
REFERENCES
1. Wagoner MD, Cox TA, Ariyasu RG, et al. Intraocular lens implantation in the absence of capsular support: A report by the American Academy of Ophthalmology. Ophthalmology 2003;110:840–859.
2. Shen JF, Deng S, Hammersmith KM, et al. Intraocular lens implantation in the absence of zonular support: An outcomes and safety update. Ophthalmology 2020;127:1234–1258.
3. Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the adult eye preferred practice pattern. Ophthalmology 2022;129:P1–P126.
4. Kaufmann GT, Boucher N, Sharma C, Starr MR. Trends in secondary intraocular lens surgery among vitreoretinal surgeons. Oph Retina 2023;7:965–971.
5. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology 2017;124:1136–1142.
6. Price MO, Price FW, Werner L, et al. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg 2005;31:1320–1326.
7. Medin H, Kure ISH, Dalby M, et al. Long-term risk of suture breakage after scleral fixation of late in-the-bag intraocular lens dislocation with a polypropylene 10-0 suture. J Cataract Refract Surg 2022;48:1408–1412.
8. Drummond SC, Feist JE, Crosson JN, et al. Scleral fixated secondary IOLs: An outcomes comparison between the Yamane and Gore-Tex-sutured techniques. Ophthalmic Surg Lasers Imaging Retina 2024:1–7.
9. Hayashi K, Hayashi H, Nakao F, Hayashi F. Intraocular lens tilt and decentration, anterior chamber depth, and refractive error after trans-scleral suture fixation surgery. Ophthalmology 1999;106(5):878-82.
10. Choi JY, Han YK. In-and-out technique for intraocular lens scleral fixation. Ophthalmology 2018;12:1279–1284.
11. Patel KG, Yazdani A, Abbey AM. Twenty-five and twenty-seven-gauge sutureless intrascleral fixation of intraocular lenses: Clinical outcomes and comparative effectiveness of haptic flanging in a large single-surgeon series of 488 eyes. Retina 2021;41:2485–2490.
12. Byun Z, Kong M, Son G. Intraocular lens malposition after sutureless intrascleral fixation of intraocular lens. Retina 2022;42:64–72.
13. Todorich B, Stem MS, Kooragayala K, et al. Structural analysis and comprehensive surgical outcomes of the sutureless intrascleral fixation of secondary intraocular lenses in human eyes. Retina 2018;38:S31–S40.
14. Kelkar N, Eid K, Nakatsuka AS, et al. Severe intraocular lens tilt after the Yamane technique. J Cataract Refract Surg 2025;51:126–132.
15. Ripa M, Angunawela R, Motta L. Scleral fixation of Carlevale intraocular lens: A systematic review and meta-analysis. Retina 2023;43:1750–1762.
16. Meshkin RS, Hoffman SE, Chaaya Md C, et al; American Society of Retina Specialists Health Economic Committee. Time-driven, activity-based cost analysis of secondary intraocular lens implantation. J Vitreoretin Dis. April 6, 2026 [Epub ahead of print.]



