Take-home points
|
 |
Bio Dr. Adam is the chair of clinical research at Colorado Retina Associates and an adjunct clinical associate professor at Rocky Vista University. |
Having trained just under a decade ago, I've been lucky to bear witness to and take part in the evolution of secondary IOLs. ACIOLs, scleral- fixated IOLs with prolene and Gore-tex suture fixation, and sutureless intrascleral flanged haptic fixation (in that order) represent the progressive iteration of vitreoretinal surgical innovation for eyes without capsular support. An optimal surgical approach for an individual case might be best approached with any of these techniques, but in my hands, intrascleral flanged haptic fixation has provided simultaneous simplicity, predictability and versatility that make it my go-to approach for secondary IOL fixation.
First conceived of and published by Shin Yamane and colleagues in 2017, the flanged intrascleral IOL fixation with double-needle technique was the last transformative surgical approach for secondary IOL implantation since Gore-tex suture fixation.1 As someone who was formally trained during residency and fellowship to implant ACIOLs and scleral fixate AO60s and MX60s (Bauch + Lomb, Vaughan, Ontario Calif.) with Gore-tex suture, no love is lost for the latter technique. Smaller corneal incisions, a one-size-fits-all approach, less risk of endothelial failure and glaucoma, and a more physiologic placement of the IOL behind the iris plane are clear advantages of Gore-tex fixation over ACIOLs. I started my post-fellowship career using this technique, but once I became familiar with sutureless flanged intrascleral fixation, there was no going back.
| Read the counterpoint article here. |
What first attracted me to sutureless secondary IOL fixation was obvious to me from the first case I performed in 2017. No sutures! If I wanted to suture, I would have pursued a glaucoma fellowship. One of the most challenging pain-points of the Gore-tex fixation technique relates to all the suturing it takes to finish a case. Between the conjunctival peritomy, corneal incision and sclerotomy sites, the opportunities for suturing in these cases are frankly too frequent. Furthermore, even when every potential suture is placed, the risk of post-operative hypotony is still quite high at approximately 10 percent.2 The beauty of sutureless flanged haptic fixation is that the haptics are secured in 30-gauge beveled sclerotomies, compared to four separate 25- or 27-gauge sclerotomies for Gore-tex suture fixation, significantly reducing the relative risk of postoperative hypotony.
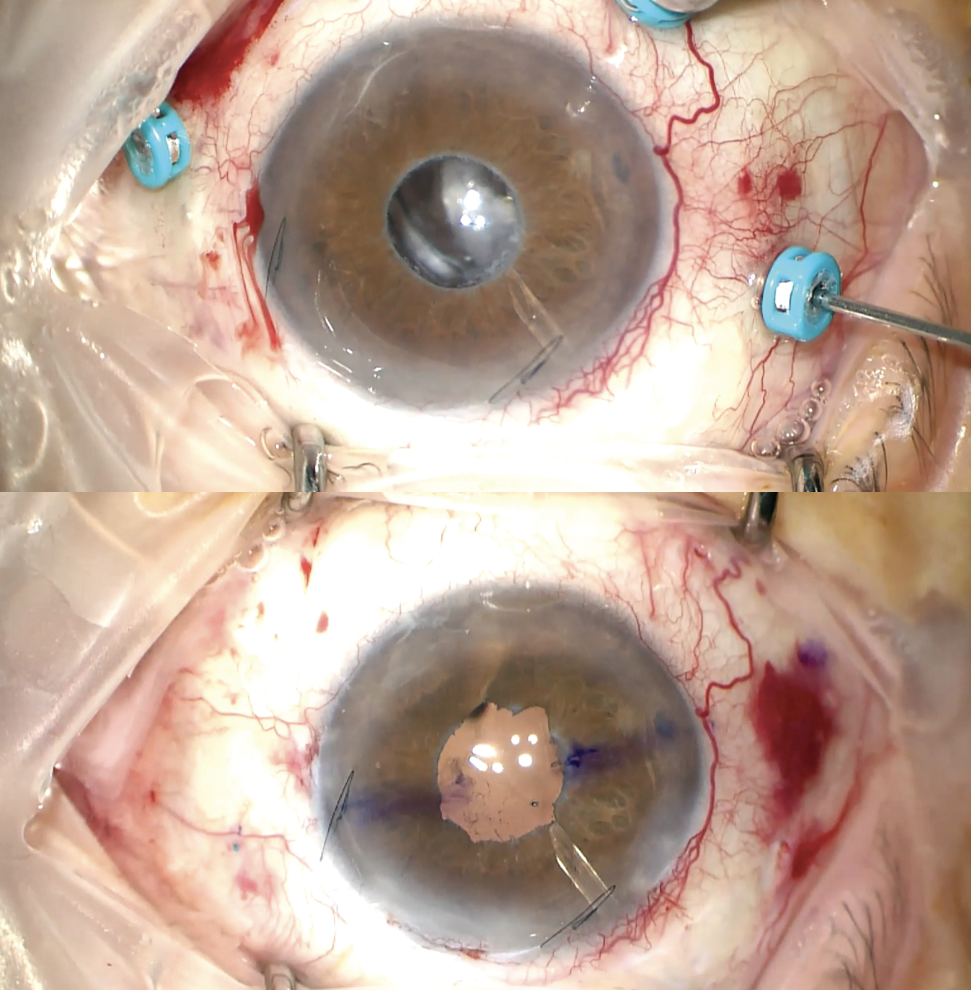 |
| Figure 1. A patient with a subluxed IOL in the setting of advanced pseudoexfoliation glaucoma, a small pupil and a history of tube shunt and Xen stent placement (top). Conclusion of the case with a well-centered scleral fixated IOL, all without sutures (bottom). |
In eyes with complex anterior segment pathology, Gore-tex fixation can present even more challenges over sutureless intrascleral flanged haptic fixation. In an eye with compromised conjunctiva from topcical glaucoma treatment and limited scleral real-estate from prior incisional glaucoma surgery, the thought of dissecting and suturing conjunctiva with a Gore-Tex fixation technique seems barbaric compared to a sutureless tranconjunctival approach. I was faced with this very clinical scenario in an 80-year-old patient with a subluxed IOL, advanced pseudoexfoliation glaucoma, and a history of tube shunt and Xen stent placement. Adding insult to injury, pupillary dilation for this patient was quite poor (Figure 1). In cases like these, the limited surgical trauma induced by needle-assisted flanged haptic fixation makes what would be a complex sutured IOL case to be a rather straightforward secondary IOL case, with an excellent and predictable anatomic outcome.
I often find myself grateful for having this sutureless technique in my armamentarium in cases where there's a history of trauma, scleral buckle and scleromalacia that would present more of a challenge with a sutured technique over a sutureless technique. The simplicity of the technique allows the surgeon to avoid taking down conjunctiva/Tenon's and finding four sclerotomy sites suitable for suture passes.
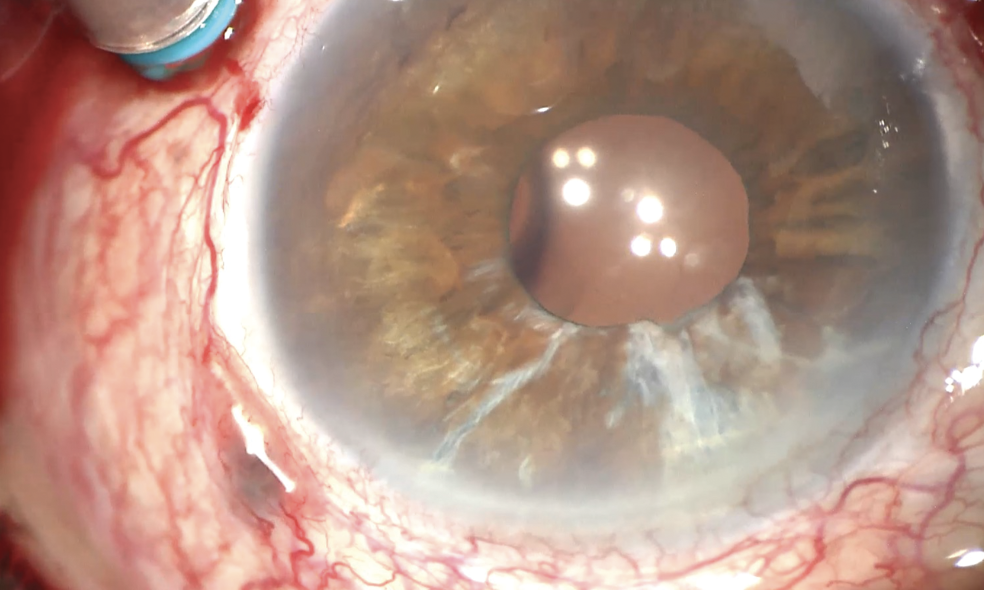 |
| Figure 2. Scleral-fixated Akreos A060 with exposed temporal Gore-tex suture prior to exchange with a scleral-fixated three-piece IOL. |
Over the years, I've explanted a number of Gore-tex fixated IOLs for a variety of reasons, including conjunctival erosion (Figure 2), eyelet fracture of an MX60, and opacification of the hydrophilic AO60.3,4 These examples highlight a number of known and well described complications of the Gore-tex technique. Fortunately, a sutureless flanged haptic fixation technique provides an ideal solution for all these sutured technique complications.
One of the most attractive aspects of the sutureless flanged haptic fixation technique is the flexibility of IOL selection options available. This, of course, can present unexpected challenges as we've seen with the “rotisserie” tilt of the CT Lucia 602 (Zeiss, Oberkochen, Germany).5 However, lenses that I've found suitable for this technique include the AR40 (AMO), LI61AO (Bauch + Lomb) and previously implanted 3-piece PMMA lenses, as rescue and scleral fixation avoids the need for a large incision for explantation.6 Furthermore, I've found great success in using the RxSight Light Adjustable Lens (LAL) to maximize refractive outcomes in patients with specific refractive goals and/or a history of prior corneal refractive surgery.7 Refractive outcomes with the LAL appear to be significantly better and more predictable than scleral-fixated toric IOLs with a sutured approach.8
Regardless of the technique used, it's important for surgeons who perform secondary IOL cases to be aware of the steep learning curve when trying a new approach and to be versed in multiple techniques so that the ideal approach for each unique surgical scenario is applied. We've come a long way in treating eyes without capsular support, and it's been exciting to see how these evolving sutureless techniques have allowed retina specialists to be more refractive-minded. In the near future, even more lens options may be available for these patients; an artificial lens capsule device (LensOne, Long Bridge Medical) is currently in clinical trials for sutureless scleral fixation. More than achieving an “anatomic” success, our field is now striving for refractive success in these complex eyes. RS
REFERENCES
1. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology 2017;124:8:1136-1142.
2. Khan MA, Gupta OP, Smith RG, Ayres BD, Raber IM, Bailey RS, Hsu J, Spirn MJ. Scleral fixation of intraocular lenses using Gore-Tex suture: Clinical outcomes and safety profile. Br J Ophthalmol 2016;100:5:638-43.
3. Forlini M, Dell’aversana G, Bratu A Rossini P, Cavallini G, Forlini C. Akreos Adapt AO Intraocular Lens Opacification: A Case Report. Case Reports In Ophthalmology 2013;4:151-4.
4. Gupta, R. Rishi et al. Dislocation of a scleral-fixated, hydrophobic, single-piece acrylic intraocular lens secondary to eyelet fracture from Gore-Tex suture. Journal of VitreoRetinal Diseases 2019;3:395-398.
5. Zhang A, Dipen K, Tan J, Adam MK. Axial instability of the Zeiss CT Lucia 602 intraocular lens with transconjunctival intrascleral haptic fixation. American Society of Retina Specialists Annual Meeting; Seattle, WA; July 31, 2023.
6. Curran C, Adam MK. Clinical and anatomic outcomes of 3-piece poly(methyl methacrylate) intraocular lens rescue and needle-assisted transconjunctival intrascleral lens fixation. J Vitreoretin Dis 2023;7:5:404-411.
7. Ton NS, Kruger M, Adam MK. Combined pars plana vitrectomy and novel scleral fixation of the Light Adjustable Lens. Retina 2025 Jan 17.
8. Ward MS, Hou AC, Murphy DA, Schmutz MA, Riaz KR. Scleral fixation of a toric lens to treat corneal astigmatism in eyes without capsular support. Clinical Ophthalmology 2021;15:2317-2325.



