
 |
Bios Dr. Nogueira is a surgical retina fellow at the University of Montreal. |
Refractory macular holes, especially after prior internal limiting membrane peeling, are often challenging, with reoperation success rates varying from 46.7 to 68.9 percent and suboptimal visual outcomes.1,2 MH size is crucial for primary success rates as holes <400 µm have near 100-percent closure, while larger holes (>400 µm) reach 80 percent.3 Emerging techniques including macular hole hydrodissection,4 human amniotic membrane grafts5 and autologous retinal transplantation show promise for large or recurrent MHs, especially those >800 µm.6
ART, in particular, has shown encouraging results, significantly improving both visual acuity and closure rates in refractory and large MHs, with minimal reported complications.7 However, the ART procedure is technically challenging and optimizing preoperative assessment and surgical technique is crucial for success.
Here we outline our 10 tips for enhancing the success of ART:
1. Use of chandelier endoillumination. The bimanual approach with a chandelier is helpful in our experience for better graft manipulation and tissue positioning.
2. Mobilizing MH borders. Viscodissection of the MH borders with an appropriate cannula (Synergetics) helps in positioning the graft beneath the hole’s edges. A similar technique has been described with the use of macular hole hydrodissection4,8 to free the edges of the macular hole and allow for the graft to be inserted under the shelf created. This step helps in ensuring the stability of the graft intra- and postoperatively (Figure 2).
 |
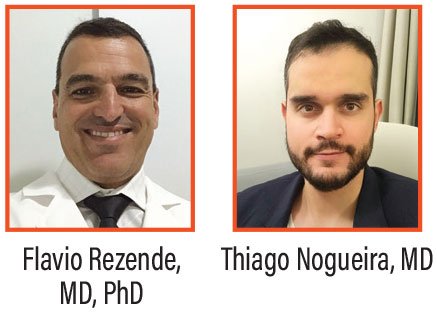
| Figure 1. (A) Intraoperative images demonstrating initial measurement of the macular hole with intraoperative-OCT, (B) followed by measurement of the graft with iOCT. (C) Next, viscodissection of the MH borders is completed to create a space for insertion of the graft. (D) Laser markings are used as a guide for graft sizing, and (E) perfluorocarbon is placed anterior to the graft harvesting site. (F) The graft is obtained with microscissors and viscodissection and (G) transported to the MH site using a Flex Loop (H) and Maxgrip forceps (I), where it’s positioned at the borders of the graft underneath the edges of the MH with the Maeno-Awh Super Manipulator. |
3. Graft harvesting site. We prefer to collect the graft from the midperipheral nasal retina, as previous histological studies have demonstrated a higher cone concentration of photoreceptors in this location compared to other quadrants.9 This feature makes the midperipheral nasal retina a desirable tissue for macular transplantation.
4. Intraoperative measurements and marking the graft. Intraoperative OCT or a Finesse Flex Loop (Alcon) may be used for measuring the MH and the graft size. The graft should be slightly bigger than the MH measurement. This will allow for the graft to be placed under the macular hole edge.
With the use of intraoperative OCT, we also measure the size of the graft to be harvested (Figure 1). We use four laser marks placed at the midperipheral nasal retina to outline the donor bed for graft harvesting. In our opinion, cautery should be avoided as it may damage the graft edges, which are believed to be important for proper integration with the macular hole borders.
5. Use of perfluorocarbon liquids for the donor bed. The use of perfluorocarbon liquids plays a crucial role in stabilizing the donor bed during the retinal graft harvesting process. These high-density, optically clear liquids provide a tamponade effect that serves multiple functions.
First, PFCL facilitates stabilization of the retinal tissue, preventing inadvertent movement of the donor graft during dissection. By fully covering the donor bed, it creates a mechanical barrier that minimizes traction on surrounding retinal structures, reducing the risk of unintentional displacement or fragmentation of the graft.
Second, PFCL serves as an effective hemostatic agent. Its high specific gravity reduces the likelihood of hemorrhage during graft extraction as it mitigates the risk of bleeding from fine retinal or choroidal vessels by allowing controlled cauterization if necessary.
 |
| Figure 2. (A) Preoperative OCT of a giant macular hole (minimum hole diameter: 1,511 µm) in a patient with multiple failed prior surgeries, including ILM peeling, macular hole border hydrodissection with BSS and amniotic membrane transplantation. Preoperative visual acuity was counting fingers at 1 foot, with a large central scotoma. The white arrowhead indicates the displaced amniotic membrane after intraocular gas reabsorption. (B) One week post-autologous retinal transplant, with perfluorocarbon heavy liquid as a temporary tamponade. Initial graft integration is observed and visual acuity improved to counting fingers at 4 feet. (C) Three weeks post-ART. PFCL was removed two weeks after ART, and air was used as tamponade for the second surgery. OCT shows further graft integration at the hole’s border, with BCVA improving to 20/200. The patient also reported a significant reduction in the central scotoma. |
6. Dissection of the graft from the donor bed. After making the initial snip at the most posterior laser mark with microscissors, dispersive viscoelastic is injected to facilitate dissection of the graft from the donor bed, making it easier to cut the tissue using either microscissors or vitrector. While the vitrector offers a more ergonomic approach, microscissors provide greater precision for accurately sizing the graft.
After the graft is removed, laser should be applied to the borders of the donor bed to ensure proper retinopexy and achieve hemostasis to prevent any potential bleeding.
7. Transportation of the graft to the macular hole. The graft is transported to the macular hole under perfluorocarbon using microforceps (e.g., Maxgrip, Alcon), a supermanipulator (Maeno-Awh Super Manipulator, Katalyst), or a Finesse Flex Loop (Alcon). The advantage of using microforceps is that they don’t apply pressure to the retinal surface; however, the graft may adhere more readily to the forceps than to the supermanipulator, making graft positioning more difficult.
8. Graft positioning underneath the MH edges. The graft can be positioned either on top of the macular hole or tucked beneath its borders. Placing the graft underneath the borders offers greater stability and allows for fluid-air exchange, enabling the use of long-acting gas tamponade. However, this approach involves more manipulation and carries a risk of additional retinal trauma.
When the graft is positioned on top of the macular hole, we recommend avoiding fluid-air exchange. Using perfluorocarbon as tamponade for two weeks postoperatively reduces the risk of graft dislocation. The choice of strategy is at the surgeon’s discretion. For holes larger than 1,500 µm, positioning the graft on top of the macular hole with perfluorocarbon tamponade may be the most effective option.6
9. Fluid air-exchange and PFCL removal. If fluid-air exchange is performed, we recommend positioning the infusion line horizontally toward the anterior vitreous cavity to minimize turbulence at the PFCL-air interface and reduce the risk of graft displacement. Tilting the eye superiorly during FAX can also be helpful.
During this phase, it’s crucial to closely monitor the graft’s position, as even slight movements may indicate a high risk of postoperative displacement. If this occurs, we recommend repositioning the graft and injecting PFCL for tamponade without returning to fluid, which increases the likelihood of maintaining proper graft placement.
When using PFCL as a tamponade, it’s essential to ensure that no BSS meniscus remains, as this can increase the risk of graft displacement. The PFCL should be injected until reflux is observed through the infusion and cannulas, confirming that no BSS is left in the eye.
10. Postoperative positioning. When using C3F8 as a tamponade, most specialists recommend facedown positioning for several days up to a week.6 However, we prefer an upright position, as we believe it provides comparable graft stabilization while offering greater comfort for the patient. In cases where PFCL is the tamponade of choice, the literature suggests maintaining a dorsal decubitus position for up to a week.6 In contrast, we advocate for a shorter duration of 24 hours post-surgery dorsal decubitus is enough for graft stabilization, provided that a proper PFO fill was achieved at the end of the procedure.
Bottom Line
ART has emerged as a promising option for large and refractory macular holes, offering good anatomical and functional outcomes when conventional techniques fail. Success with ART relies on surgical planning, donor site selection, graft sizing and handling, and intra- and postoperative management to minimize complications and maximize stability. The 10 pearls outlined in this article may serve as a valuable tool in the surgical management of challenging macular holes. RS
References
1. Moisseiev E, Fabian ID, Moisseiev J, Barak A. Outcomes of repeated pars plana vitrectomy for persistent macular holes. Retina 2013;33:6:1137–1143.
2. D’Souza MJ, Chaudhary V, Devenyi R, Kertes PJ, Lam WC. Re-operation of idiopathic full-thickness macular holes after initial surgery with internal limiting membrane peel. Br J Ophthalmol 2011;95:11:1564–1567.
3. Rezende FA, Ferreira BG, Rampakakis E, et al. Surgical classification for large macular hole: Based on different surgical techniques results: The CLOSE study group. Int J Retina Vitreous 2023;30:9:1:4.
4. Felfeli T, Mandelcorn ED. Macular hole hydrodissection: Surgical technique for the treatment of persistent, chronic, and large macular holes. Retina 2019;39:4:743-752.
5. Rizzo S, Caporossi T, Tartaro R, et al. A human amniotic membrane plug to promote retinal breaks repair and recurrent macular hole closure. Retina 2019;39:S95–S103.
6. Grewal DS, Charles S, Parolini B, Kadonosono K, Mahmoud TH. Autologous retinal transplant for refractory macular holes: Multicenter international collaborative study group. Ophthalmology 2019;126:10:1399-1408.
7. Lee PY, Chang YC, Liu PK, et al. Long-term follow-up of refractory large macular hole with autologous neurosensory retinal free flap transplantation. J Ophthalmol 2022;9:2022:1717366.
8. Felfeli T, Corrin M, Papanikolaou J, Mandelcorn ED. Macular hole hydrodissection technique with human amniotic membrane for repair of large macular holes. Retina Cases Brief Rep 2023;1:176:767-770.
9. Curcio CA, Sloan KR, Kalina RE, Hendrickson AE. Human photoreceptor topography. J Comp Neurol 1990;22:292:4:497-523



