
 |
Bios |
Optic disc maculopathy can result in serous macular detachment and progressive vision loss. Surgical intervention aims to eliminate subretinal fluid accumulation, restore the macular architecture, and stabilize visual outcomes. Given the rarity of the condition, there currently no universally accepted surgical approach for management.1 Pars plana vitrectomy with release of vitreoretinal traction and gas tamponade has emerged as the most widely used strategy, with additional maneuvers such as internal limiting membrane peeling, laser photocoagulation, inverted ILM flap or tissue plugging used selectively to block fluid egress through the pit.1-3 More recently, autologous scleral grafting has been described as a means of creating a mechanical seal at the optic disc pit, with encouraging anatomical and functional outcomes in selected cases.4,5
Here, we review a structured approach to managing optic disc maculopathy, with a focus on scleral graft placement and other intraoperative techniques.
Preoperative Assessment
Preoperative optical coherence tomography imaging is critical to evaluate the extent of macular involvement, the level of subretinal fluid, and the pit’s exact location. Imaging insights guide the surgical plan and scleral graft dimensions.
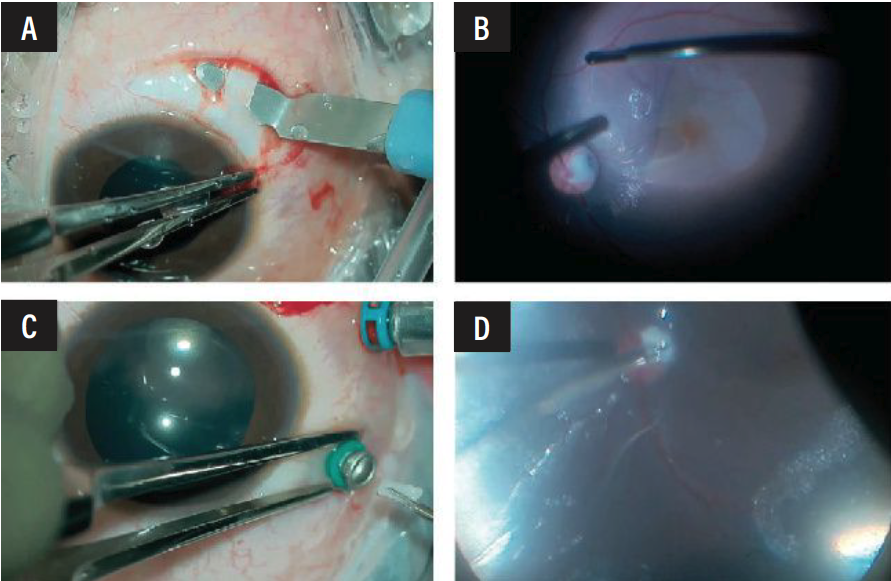 |
| Adequate size and thickness of the scleral graft is dissected and prepared (A). Following ample ILM peeling (B), the scleral graft inserted through a 23G vitrectomy port (C) and gently inserted into the optic disc pit (D). |
Intraoperative Techniques
Following are the steps for achieving a good result:
1. Generous peritomy. Begin with a peritomy to adequately expose the scleral graft harvesting site, ensuring easy access for graft preparation.
2. Scleral graft preparation. Mark the appropriate size and thickness for the graft, then carefully dissect and prepare it for insertion later in the surgery.
3. Pars plana vitrectomy and PVD induction. Perform a pars plana vitrectomy, followed by posterior vitreous detachment induction. This helps reduce vitreoretinal traction around the optic disc.
4. Internal limiting membrane peeling. Conduct a thorough ILM peel around the macula to assist in the redistribution of subretinal fluid and alleviate tangential traction.
5. Fluid-air exchange. Switch to fluid-air exchange to create a stable environment for graft insertion. Ensuring an air-filled vitreous cavity enhances graft positioning and reduces fluid ingress.
6. Port exchange to 23G. Change the dominant port to 23G to facilitate smooth insertion of the prepared scleral graft.
7. Harvesting and insertion of the scleral graft. Retrieve the pre-prepared scleral graft. Insert it through the 20 G port, switching hands may be necessary for precise alignment.
8. Graft positioning. Using gentle movements, guide the graft into the optic disc pit and secure it in place under air. Further drying of the vitreous cavity ensures the graft remains stable.
9. Endotamponade with SF6. Inject SF6 gas to provide endotamponade, helping to maintain graft positioning and prevent fluid re-accumulation. Instruct patients on face-down positioning postoperatively to optimize graft contact.
Postoperative Management
Postoperatively, patients should maintain a face-down position to support graft adhesion and reduce subretinal fluid recurrence. Regular follow-ups with OCT imaging are recommended to monitor macular reattachment and ensure graft stability.
The Bottom Line
The combined technique of vitrectomy, ILM peeling, autologous scleral graft plugging and gas tamponade represents a logical and robust strategy for optic disc maculopathy. By addressing both tractional and communication-based mechanisms of fluid accumulation, it may improve the likelihood of durable macular reattachment in complex cases. RS
References
1. Moisseiev E, Moisseiev J, Loewenstein A. Optic disc pit maculopathy: When and how to treat? A review of the pathogenesis and treatment options. Int J Retina Vitreous 2015;1:13.
2. Iros M, Parolini B, Ozdek S, Gini G, Nawrocka ZA, Ellabban AA, Faramawi MF, Adelman R, Sallam AB; EVRS Study Group. Management of optic disc pit maculopathy: The European VitreoRetinal Society optic pit study. Acta Ophthalmol 2022;100:6:e1264-e1271.
3. Zheng A, Singh RP, Lavine JA. Surgical options and outcomes in the treatment of optic pit maculopathy: A meta-analysis and systematic review. Ophthalmol Retina 2020;4:3:289-299.
4. Babu N, Kohli P, Ramasamy K. Comparison of various surgical techniques for optic disc pit maculopathy: vitrectomy with internal limiting membrane (ILM) peeling alone versus inverted ILM flap ‘plug’ versus autologous scleral ‘plug’. Br J Ophthalmol 2020;104:11:1567-1573.
5. Shah PK, Karandikar SS, Narendran V. Scleral autograft for optic nerve head pit associated chronic maculopathy. Ophthalmic Surg Lasers Imaging Retina 2017;48:3:251-254.



