
 |
|
Bios Dr. Levinger practices at Toronto Western Hospital, University Health Network. |
Anterior-segment complications that require secondary intraocular lens fixation may often present later with posterior-segment pathology such as retinal detachment. Modern fixation techniques—scleral-sutured, sutureless intrascleral fixation, anterior iris fixation, and various IOL materials—can result in artificial physiological conditions that present challenges when surgically repairing retinal abnormalities.
When planning RD repair, tamponade selection must therefore consider not only the posterior pathology but also the material properties, position, and fluid/anterior chamber dynamics created by the specific IOL. Inappropriate tamponade choice can lead to optic opacification, pupillary block, IOP spikes, shallowing of the anterior chamber and surgical failure.
The following case illustrates how IOL fixation can dramatically influence tamponade behavior in the postoperative period.
The case
The following case demonstrates the complexity of choosing a tamponade agent in eyes with anteriorly fixated IOLs.
An 80-year-old female presented with a two-week history of vision loss in her right eye. Examination revealed a total retinal detachment with a suspected full-thickness macular hole. Her ocular history included remote cataract surgery, followed years later by bilateral IOL exchange due to subluxed IOL secondary to PXF. During those secondary procedures, anterior chamber iris-claw (Artisan) lenses were implanted in both eyes.
A pars plana vitrectomy with Densiron heavy silicone oil tamponade and 360-degree laser retinopexy were performed. Four months later, the heavy oil was removed.
At the time of oil removal surgery, the retina had persistent superior shallow residual subretinal fluid, thus 16% C3F8 gas was used as tamponade. A new inferior peripheral iridotomy was created, complementing the superior PI that had been made during the initial Artisan implantation.
Postoperative day 1
The patient presented with an intraocular pressure of 49 mmHg and a flat AC. The vitreous cavity was filled with 95% gas. Despite enlargement of the inferior PI with YAG, maximal topical therapy, and oral acetazolamide, the AC remained shallow. A vitreous gas tap was performed, reducing IOP to 7 mmHg and deepening the AC.
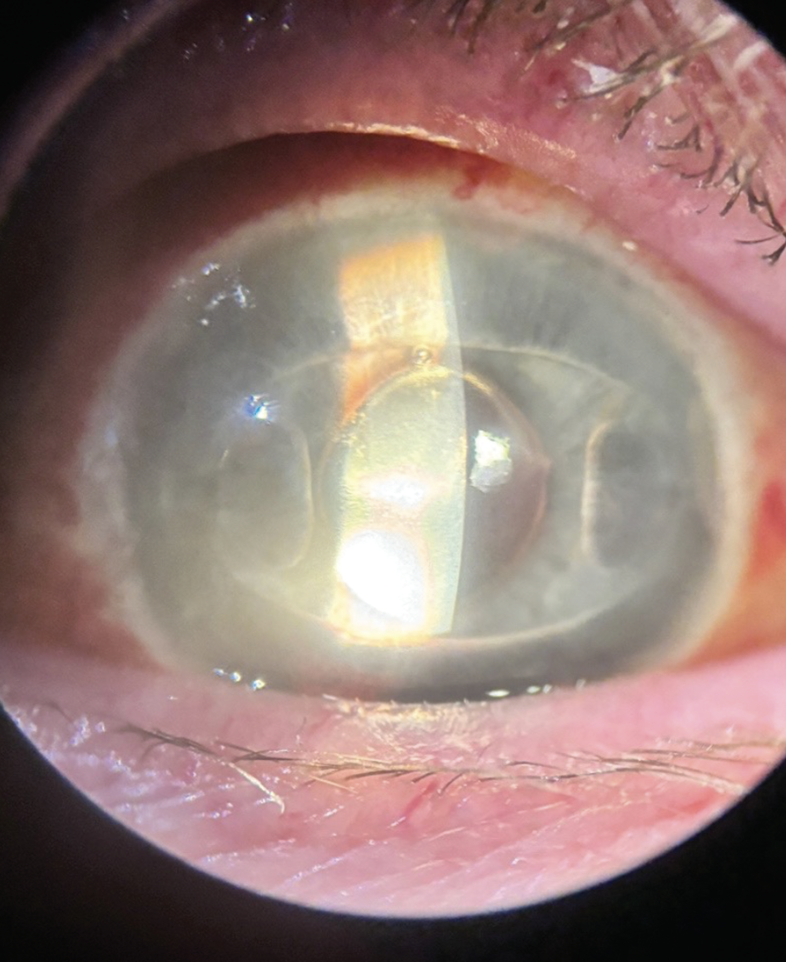 |
| Figure 1. Flat AC with Artisan IOL pushing against the cornea. |
Two days later
The patient returned with recurrent angle closure and elevated IOP with a flat AC (Figure 1). A second vitreous gas tap was required.
Day 7
Despite two vitreous gas taps, it became clear that gas tamponade in the presence of the AC clipped iris-claw IOL was preventing normal aqueous outflow and stable chamber formation. This was possibly due to a flaccid and mobile iris diaphragm that led to recurrent pupil block despite a patent PI. The patient was brought back to the OR for complete gas removal. Because the retina was now re-attached, no further tamponade was instilled.
Postoperative day 1 after gas removal
The anterior chamber was deep and the IOP had normalized.
Insight from the case
This case demonstrates that long-acting gas may be incompatible with certain anterior fixation configurations—particularly iris-claw IOLs—because even seemingly adequate PI placement may not prevent aqueous obstruction or chamber collapse.
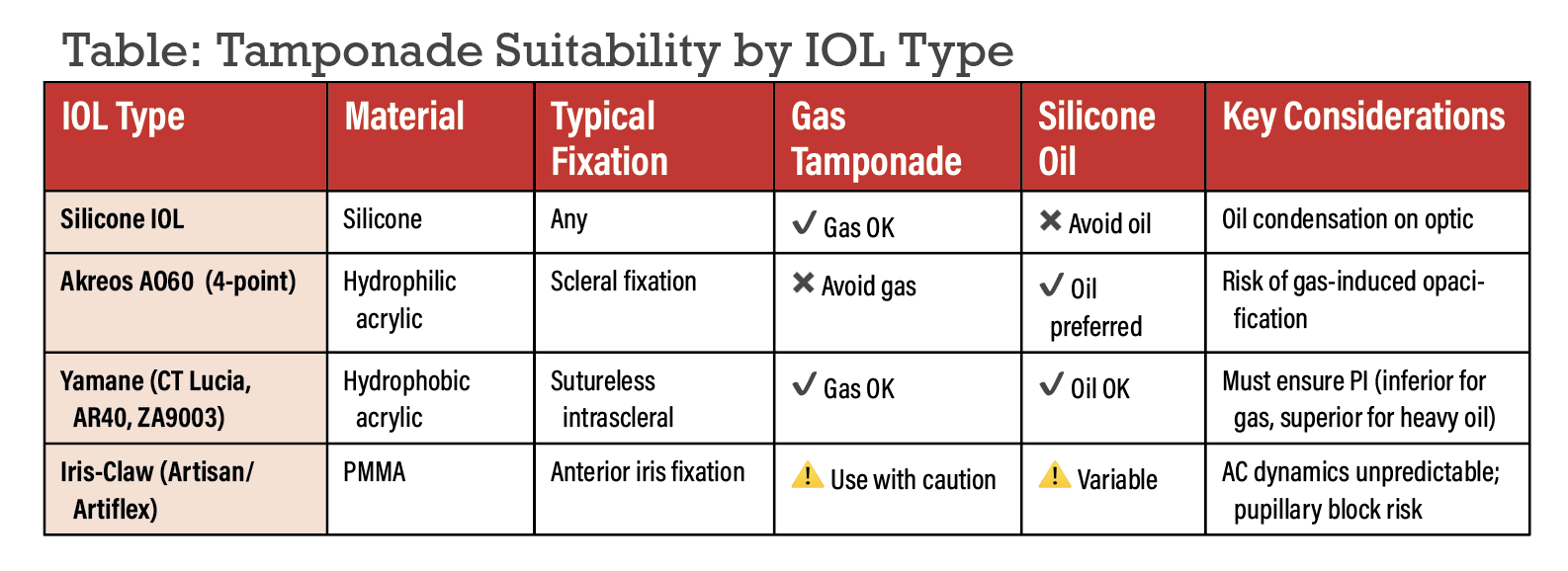 |
Tamponade considerations by IOL fixation method
Your choice of tamponade can have different levels of efficacy and pose different risks, depending on your fixation approach. Following are factors to keep in mind:
• Iris-claw (Artisan/Artiflex) and implantable collamer IOLs. Iris-claw IOLs can be placed in both the anterior and posterior chambers in aphakic eyes.1 While both lens types are indicated for aphakia without capsular support, prepupillary lenses are enclavated to the anterior mid-peripheral iris and retropupillary lenses attached behind the iris.1 Studies have found no difference in visual outcomes or in complication rates between the two groups,1,2 but prepupillary lenses possess a potential increase in corneal endothelial cell loss.1,3,4
In phakic eyes receiving IOLs, surgeons can implant Artisan/Artiflex lenses, in the AC, or implantable collamer lenses.6 ICLs are indicated in phakic eyes with moderate to high ametropia and involve placing a lens in the posterior chamber between the iris and crystalline lens.7 Gas and silicone oil tamponade are available for retinal detachment in phakic eyes with Artisan lenses or ICLs. It’s been hypothesized that long-acting gas tamponades may have increased risk of complications in phakic eyes with Artisan lenses compared to ICLs as their location can increase the risk of anterior segment complications due to factors including:6,8-10
- The AC may shallow unpredictably.
- Even multiple PIs may fail to prevent pupillary block.
- IOP may rise despite aggressive management.
- Repeated gas tapping or complete gas removal may be required.
- Artisan lenses may have increased risk of anterior segment complications with gas tamponade particularly in patients with shallow anterior chambers.11 For silicone oil tamponade, outcomes are variable and depend on iris contour, chamber depth, and outflow pathways.12,13
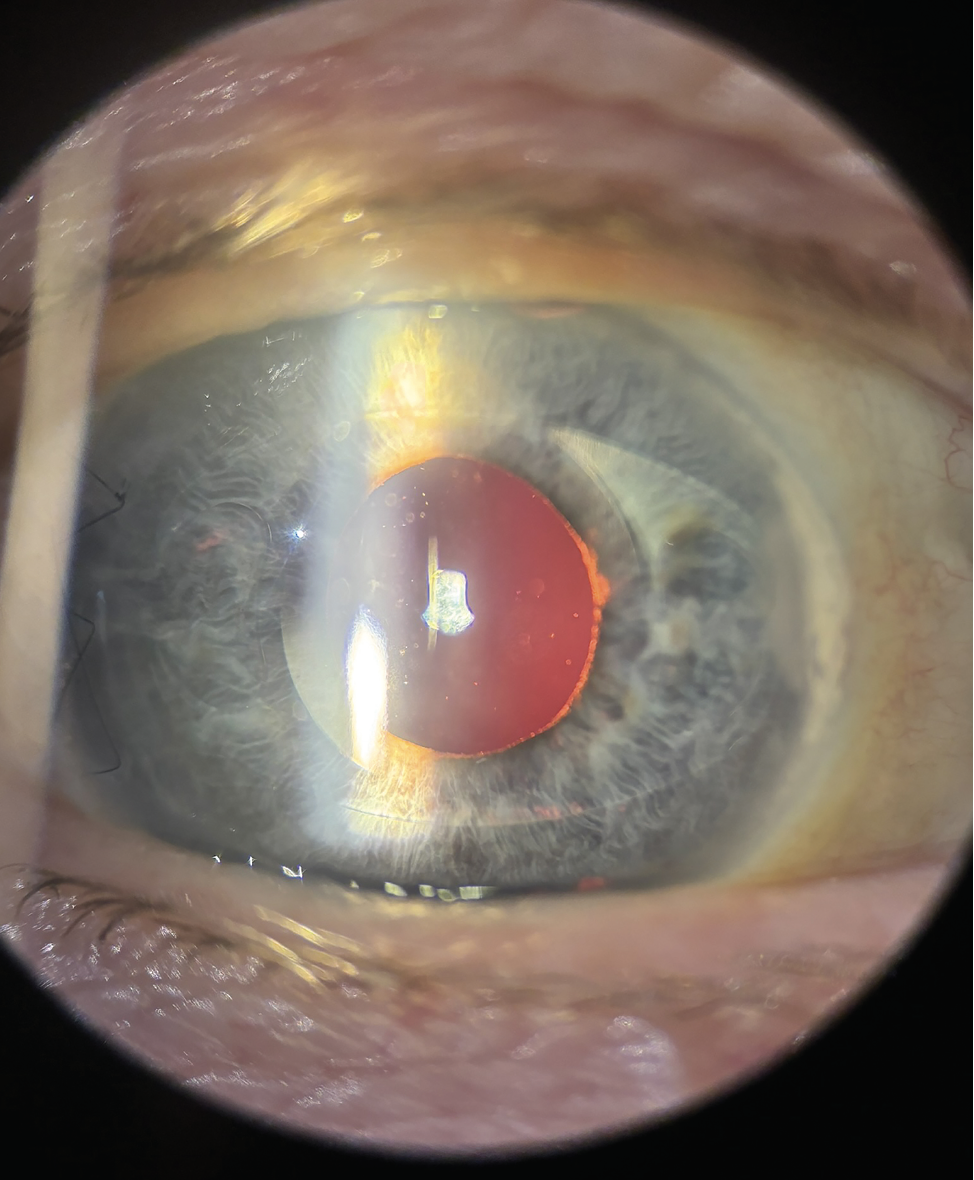 |
| Figure 2. The eye from Fig. 1 postop, after gas has been removed. |
— Practical implication: Long-acting gas tamponade should be used with caution, especially in iris-claw IOLs with shallow anterior chambers, or altered iris configuration. If possible, scleral buckle and pneumatic retinopexy may be better options in eyes with phakic IOLs.
• Silicone IOLs. These lenses are known to interact poorly with silicone oil tamponade. Silicone oil can manifest as droplets that adhere to the posterior surface of silicone lenses to reduce visual acuity.14,15 These droplets are extremely difficult or impossible to remove in both human and experimental models.14,16 F4H5 is the preferred option for reducing silicone droplets, with demonstrated clinical efficacy.17,18 While gas tamponade can cause reversible condensation in silicone IOLs, it’s preferred over silicone oil, with better functional outcomes.19,20
— Practical implication: Avoid silicone oil if a silicone IOL is present. Also consider avoiding silicone IOLs in patients at risk for vitreoretinal diseases that may require silicone oil.
• Four-point scleral fixation. This offers excellent centration and stability. However, the Akreos AO60 lens—commonly used for this technique—is a hydrophilic acrylic IOL, and this material can develop irreversible opacification when exposed to air or gas at a higher incidence than silicone or hydrophobic acrylic lenses.21-23 Rare and well-documented, opacification in hydrophilic acrylic lenses is more common in patients with Descemet stripping with automated endothelial keratoplasty, diabetes mellitus, PPV and/or glaucoma after cataract surgery.22 Preventative strategies are most important, with other lens materials chosen in patients at-risk for corneal endothelial decompensation potentially requiring intraocular gas.23
For this reason, many surgeons often choose silicone oil for RD repair in eyes with hydrophilic IOLs.
— Practical implication: Gas tamponade should generally be avoided.
• Intrascleral fixation. Hydrophobic acrylic lenses used with the Yamane technique (e.g., CT Lucia 602, Sensar AR40, ZA9003) tolerate both gas and silicone oil, and they don’t opacify in response to gas exposure.23
However, tamponade choice must consider the direction of buoyancy and the need for a proper peripheral iridotomy:
- Gas or standard silicone oil: an inferior PI prevents pupillary block.24
- Heavy silicone oil (Densiron): a superior PI is required to ensure aqueous mobility.25
— Practical implication: Compatible with all tamponades if PI placement is correct. Due to the risk of reverse pupillary block in ~30 percent of eyes treated with scleral-fixated IOL, a PI should be considered.26
 |
Summary
Tamponade selection after RD repair must take into account the type and position of anterior-segment IOL fixation:
• avoid silicone oil in silicone IOLs;
• avoid gas in hydrophilic acrylic IOLs (e.g., Akreos AO60) due to opacification risk;
• gas and oil are both acceptable in Yamane hydrophobic acrylic IOLs if the PIs are correctly positioned; and
• gas may compromise anterior chamber stability in iris-claw IOLs; consider alternative tamponades or plan for close postoperative monitoring.
A tailored approach based on the IOL material and fixation method can significantly reduce complications, ensure stable anatomical repair and improve overall outcomes. RS
References
1. Toro MD, Longo A, Avitabile T, et al. Five-year follow-up of secondary iris-claw intraocular lens implantation for the treatment of aphakia: Anterior chamber versus retropupillary implantation. PLoS One 2019;14:4:e0214140.
2. Helvaci S, Demirduzen S, Oksuz H. Iris-claw intraocular lens implantation: Anterior chamber versus retropupillary implantation. Indian J Ophthalmol 2016;64:1:45-49.
3. Peralba RT, Lamas-Francis D, Sarandeses-Diez T, Martínez-Pérez L, Rodríguez-Ares T. Iris-claw intraocular lens for aphakia: Can location influence the final outcomes? Journal of Cataract & Refractive Surgery 2018;44:7:818.
4. Schallenberg M, Dekowski D, Hahn A, Laube T, Steuhl KP, Meller D. Aphakia correction with retropupillary fixated iris-claw lens (Artisan) – Long-term results. Clin Ophthalmol 2014;8:137-141.
5. Liang IC, Chang YH, Hernández Martínez A, Hung CF. Iris-claw intraocular lens: Anterior chamber or retropupillary implantation? A systematic review and meta-analysis. Medicina (Kaunas) 2021;57:8:785.
6. Kim TI, Alió Del Barrio JL, Wilkins M, Cochener B, Ang M. Refractive surgery. Lancet 2019;393:10185:2085-2098.
7. Wannapanich T. Intraocular Implantable Collamer lens with a central hole implantation: Safety, efficacy, and patient outcomes - PMC. Accessed February 2, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC10046236/
8. Thompson. Implantable collamer lens procedure planning: A review of global approaches - PMC. Accessed February 3, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC11005927/
9. Foss. Retinal detachment following anterior chamber lens implantation for the correction of ultra-high myopia in phakic eyes - PubMed. Accessed February 3, 2026. https://pubmed.ncbi.nlm.nih.gov/8494856/
10. van der Meulen I, Gunning F, Henry Y, de Vries-Knoppert W, Gortzak-Moorstein N, de Smet MD. Management of retinal detachments in pseudophakic patients with Artisan lenses. J Cataract Refract Surg 2002;28:10:1804-1808.
11. Gopal L, Nagpal A, Kabra S, Roy J. Anterior chamber collapse following vitreoretinal surgery with gas tamponade in aphakic eyes: Incidence and risk factors. Retina 2006;26:9:1014-1020.
12. Chen J, Wang L, Tao L, Xue S, Wang Y, Wang F. Investigation of the biomechanical changes at the iris-lens interface after vitrectomy with silicone oil tamponade: Insights from ultrasound biomicroscopy. Exp Eye Res 2026;264:110855.
13. Fernández-Vigo JI, Marcos AC, Agujetas R, et al. Computational simulation of aqueous humour dynamics in the presence of a posterior-chamber versus iris-fixed phakic intraocular lens. PLoS One 2018;13:8:e0202128.
14. Apple DJ, Federman JL, Krolicki TJ, et al. Irreversible silicone oil adhesion to silicone intraocular lenses. A clinicopathologic analysis. Ophthalmology 1996;103:10:1555-1561; discussion 1561-1562.
15. Kusaka S, Kodama T, Ohashi Y. Condensation of silicone oil on the posterior surface of a silicone intraocular lens during vitrectomy. Am J Ophthalmol 1996;121:5:574-575.
16. Khawly JA, Lambert RJ, Jaffe GJ. Intraocular lens changes after short- and long-term exposure to intraocular silicone oil. An in vivo study. Ophthalmology 1998;105:7:1227-1233.
17. Liang Y, Kociok N, Leszczuk M, et al. A cleaning solution for silicone intraocular lenses: “Sticky silicone oil.” Br J Ophthalmol 2008;92:11:1522-1527.
18. Stalmans P, Pinxten AM, Wong DS. Cohort safety and efficacy study of Siluron2000 emulsification-resistant silicone oil and F4H5 in the treatment of full-thickness macular hole. Retina 2015;35:12:2558-2566.
19. Browning DJ, Fraser CM. Clinical management of silicone intraocular lens condensation. Am J Ophthalmol 2005;139:4:740-742.
20. Huang RS, Mihalache A, Lau THA, Popovic MM, Kertes PJ, Muni RH. Pars plana vitrectomy with silicone oil or gas tamponade for uncomplicated retinal detachment: A systematic review and meta-analysis. Am J Ophthalmol 2024;266:144-155.
21. Darcy K, Apel A, Donaldson M, et al. Calcification of hydrophilic acrylic intraocular lenses following secondary surgical procedures in the anterior and posterior segments. Br J Ophthalmol 2019;103:12:1700-1703.
22. Fernández J, Sánchez-García A, Rodríguez-Vallejo M, Piñero DP. Systematic review of potential causes of intraocular lens opacification. Clin Exp Ophthalmol 2020;48:1:89-97.
23. Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the adult eye preferred practice pattern. Ophthalmology 2022;129:1:P1-P126.
24. Zalta AH, Boyle NS, Zalta AK. Silicone oil pupillary block: An exception to combined argon–Nd:YAG laser iridotomy success in angle-closure glaucoma. Arch Ophthalmol 2007;125:7:883-888.
25. Pavlidis M, Scharioth G, De Ortueta D, Baatz H. Iridolenticular block in heavy silicone oil tamponade. RETINA 2010;30:3:516.
26. Schranz M, Schartmüller D, Lisy M, Reumueller A, Abela-Formanek C. Reverse pupillary block, in contemporary scleral intraocular lens procedures. Clin Exp Ophthalmol 2024;52:6:644-654.



