
 |
Bios Dr. Sosa is a vitreoretinal surgeon, associate professor at the Retina Department at Hospital Dr. Elias Santana (CCSM), Santo Domingo, Dominican Republic. Financial disclosure: none. Dr. Franklin is a retina specialist at the Diagnostic and Medical Clinic, Mobile, Alabama. Financial disclosure: Consultant (Alcon, AsclepiX, Neuracle, OcuTerra, Outlook Therapeutics); Founder/CEO (ForwardVue Pharma). (Cont’d, next page) Dr. Flores is a retina and vitreous surgery fellow at Hospital Dr. Elias Santana (CCSM), Santo Domingo, Dominican Republic. Financial disclosure: None Dr. Dominguez is a vitreoretinal surgeon and associate professor at the Retina Department at Hospital Dr. Elias Santana (CCSM). Financial disclosure: none Dr. Abreu is a vitreoretinal surgeon, and associate professor at the Retina Department at Hospital Dr. Elias Santana (CCSM). Financial disclosure: Consultant (Alcon, Bayer, Genentech/Roche). |
Vitreous hemorrhage is a common complication and cause of persistent visual loss after surgery for proliferative diabetic retinopathy with a reported incidence ranging from 20 to 75 percent.1,2 Early postoperative vitreous hemorrhage, occurring in the first four weeks, is caused either by postoperative leakage of the remnant vessels or dissected tissue or by lysis of residual blood in the cavity.3
|
|
Figure 1. Adapted optical exciter filter. |

Early postoperative vitreous cavity hemorrhage, which occurs within the first few days after surgery, hinders visual recovery due to its persistence and lack of clearance. It can lead to elevated intraocular pressure and can make further treatment for diabetic retinopathy difficult.3 Although spontaneous resolution occurs in most cases, non-clearing postoperative vitreous cavity hemorrhage requires revision surgery in 10 percent of the cases to address any underlying causes.4
Intraoperative fluorescein angiography enables detection of residual retinal neovascularization as active leakage which may be treated with laser or diathermy. This will, in turn, reduce the risk of early postoperative vitreous cavity hemorrhage and expedite visual recovery, reduce complications and improve surgical outcomes for patients.
Surgical management and practical tips for intraoperative FA
This is the case of a 56-year-old male with a longstanding vitreous hemorrhage and proliferative diabetic retinopathy. Preoperative vision was hand motion. A conventional 25G pars plana vitrectomy was performed. After initial vitrectomy, ILM peeling was executed at the macular area and the attached nasal hyaloid was addressed completing the procedure.
In this case, a classic intraoperative FA image was obtained with a 485 nm bandpass filter installed on the light module of our Constellation vitrectomy system. The barrier filter was achieved digitally with the Alcon NGenuity visualization system, creating a new filter and modifying the color, saturation, contrast and hue to enhance the green and produce a grayscale image similar to the in-office FA.
 |
|
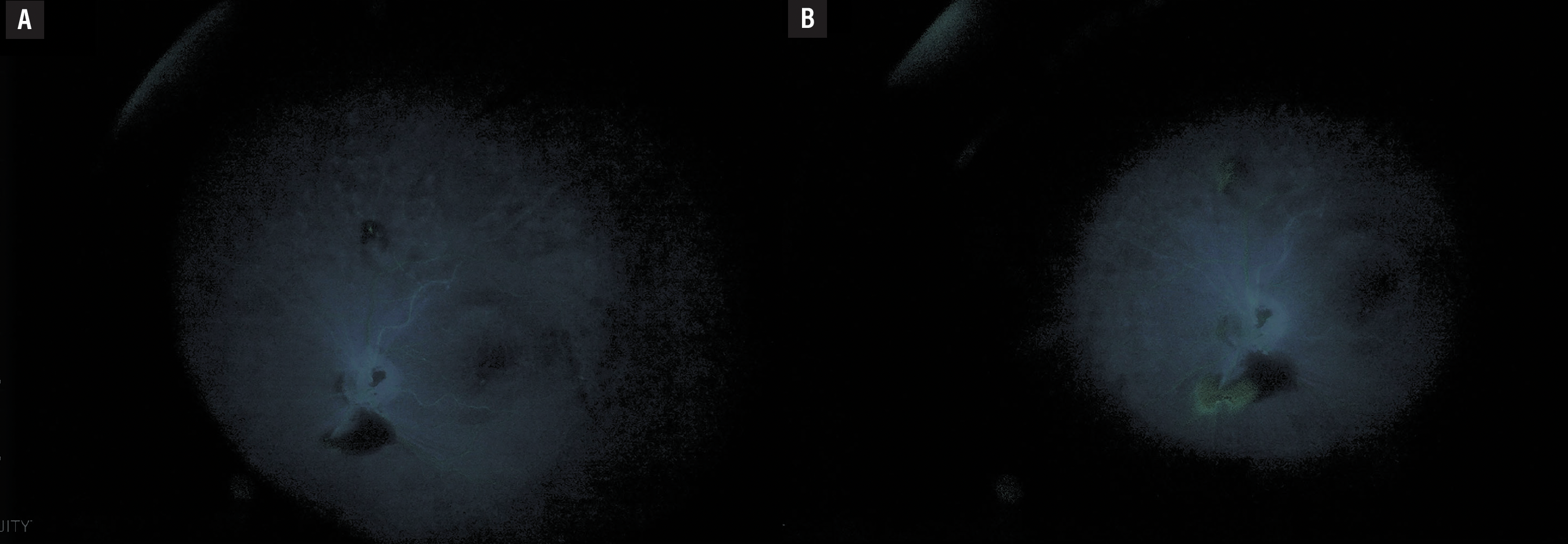
Figure 2. (A) Early intraoperative angiography phases (10 seconds). (B) Late intraoperative angiography phases (90 seconds). |
Prior to administration, the IOP was lowered to less than 30 mmHg to facilitate faster fluorescein entry into the eye and enhance image quality. The intravenous fluorescein was injected firmly with a constant speed over five to seven seconds. The iris camera was opened, and the gain was adjusted to improve image brightness. With the aid of the intravenous fluorescein, leaking vessels were identified, and continuous endolaser was applied to promote accurate hemostasis with less damage to the surrounding tissue.
At postoperative month three, the patient preserves a BCVA of 20/30 in his left eye, with no complications observed during follow-up visits, thus demonstrating that intraoperative fluorescein angiography is an outstanding tool in cases of any retinal vascular disease, leading to an accurate diagnosis and faster visual recovery.
Benefits of intraoperative FA
Intraoperative FA has many benefits in vitrectomy for PDR including:
1. Identifying angiographic biomarkers such as:
a. Ischemic areas
b. Intraoperative leakage that is not evident during surgery
2. Guiding both delamination and laser in the posterior pole and the periphery.5,6
Intraoperative FA is a valuable tool for detection and management of neovascularization in patients undergoing PPV for proliferative diabetic retinopathy. RS
REFERENCES
1. Tan SZ, Steel DH, Stanzel BV, et al. Safety and effectiveness of pre-emptive diabetic vitrectomy in patients with severe, non-fibrotic retinal neovascularisation despite panretinal photocoagulation. Eye (Lond). 2023;37:8:1553-1557.
2. Khuthaila MK, Hsu J, Chiang A, et al. Postoperative vitreous hemorrhage after diabetic 23-gauge pars plana vitrectomy. Am J Ophthalmol. 2013;155:757-63, 763.e1-2.
3. Smith JM, Steel DH. Anti-vascular endothelial growth factor for prevention of postoperative vitreous cavity haemorrhage after vitrectomy for proliferative diabetic retinopathy. Cochrane Database Syst Rev. 2015;2015:8:CD008214.
4. Brown GC, Tasman WS, Benson WE, McNamara JA, Eagle RC Jr. Reoperation following diabetic vitrectomy. Archives of Ophthalmology. 1992;110:4:506‐10.
5. Cardamone M, Hüning G, Scarlett C, et al. Intraoperative angiography can efficiently identify biomarkers and guide surgical decision making. Retina. 2023;43:12:2177-2182.
6. Imai H, Tetsumoto A, Inoue S, et al. Intraoperative three-dimensional fluorescein angiography-guided pars plana vitrectomy for the treatment of proliferative diabetic retinopathy. Retina. 2023;43:359-362.



