
 |
Bios |
Intraocular cysticercosis presents unique challenges in ophthalmic surgery due to its potential to damage retinal structures and cause severe inflammation. Surgical removal aims to safely extract the cyst, reduce inflammation and preserve visual function. This video outlines a step-by-step approach to cysticercosis removal, emphasizing the necessary surgical techniques and intraoperative strategies. Coexisting complications such as retinal detachment should also be managed effectively to restore vision.
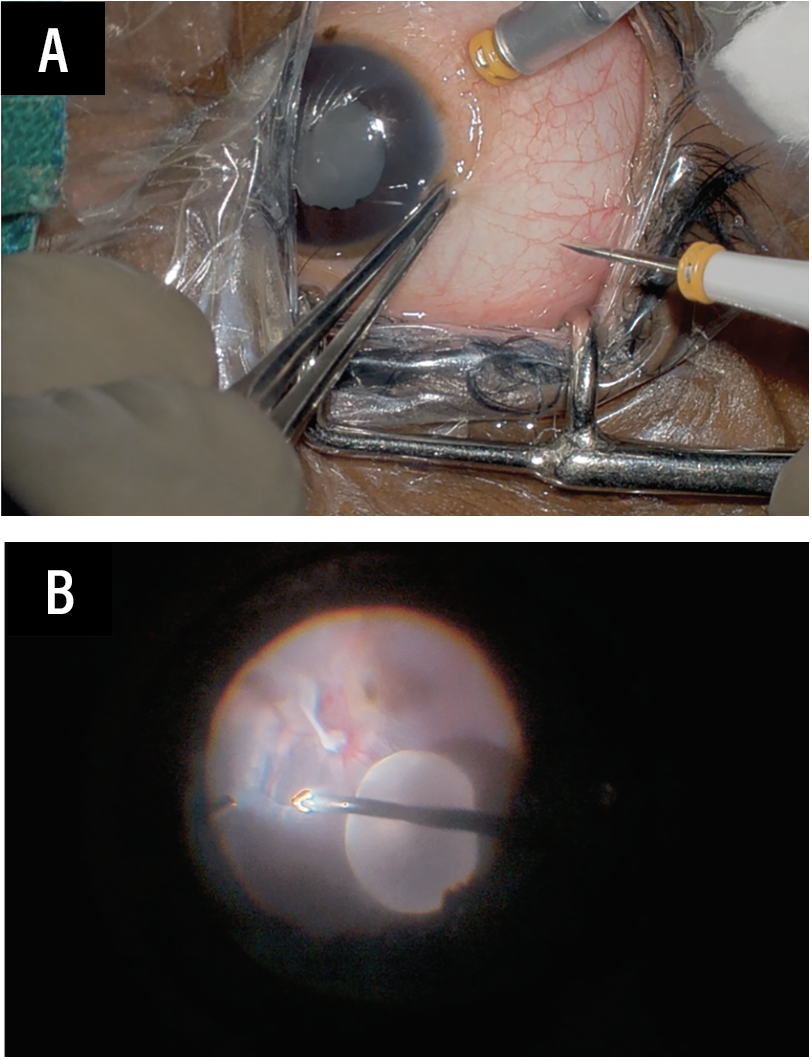 |
| Figure 1. Main port is inserted parallel and straight (A). Membrane removal is completed and the PVD is induced (B). |
Preoperative and intraoperative strategies
Preoperative imaging, such as B-scan ultrasound or optical coherence tomography, helps determine the cyst’s size, location and any associated retinal damage such as retinal detachment.
Intraoperatively, here are approaches you can use to increase the chances of a good outcome:
• Establish sclerotomy sites and place a stable infusion port to maintain intraocular pressure. The dominant port should be of straight entry and positioned parallel to the limbus to facilitate cyst removal.
• Perform a thorough vitrectomy to clear the vitreous, followed by inducing a posterior vitreous detachment for adequate exposure of the cyst.
• Carefully remove any membranes present to assist in PVD and improve visualization of the cyst and retinal layers, and to aid in managing co-existing retinal detachment.
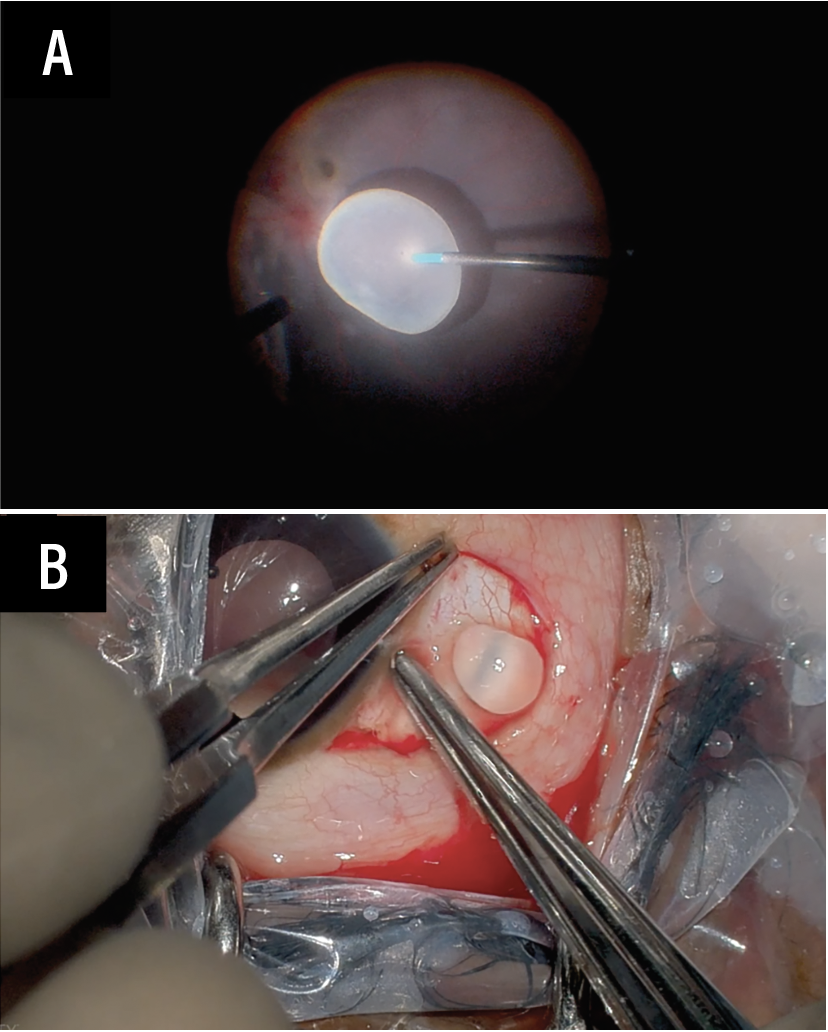 |
| Figure 2. Engagement of the cyst with soft-tip (A). Gentle pressure is applied around the sclerotomy to remove the cyst (B). |
• Perform a generous peritomy around the sclerotomy site, exposing it for smoother cyst retrieval.
• Use an MVR knife to extend the sclerotomy, providing additional space for cyst extraction.
• Use a soft-tip instrument (or blunt intraocular forceps) to gently engage the cyst. Gradually bring it closer to the sclerotomy without applying excessive force to avoid rupture.
• Apply gentle pressure around the sclerotomy site to help ease the cyst out in toto. This technique minimizes trauma and prevents cyst rupture.
• Once removed, the cyst is sent for histopathological examination to confirm diagnosis and evaluate further treatment options.
• Carefully suture the sclerotomy site to ensure it is watertight, preserving globe integrity post-procedure.
• If retinal detachment is present, perform fluid-air exchange, subretinal fluid drainage and internal limiting membrane peeling. PFCL tamponade with a silicone oil top-up can stabilize the retina, allowing for a planned second-stage vitrectomy.
• Inject intravitreal methotrexate (400 µg) to inhibit proliferative vitreoretinopathy formation, reducing the risk of recurrence and further complications.
Postoperative management
Postoperatively, a course of corticosteroids and antibiotics is recommended to control inflammation and reduce the risk of secondary infection. Close follow-up with fundus examination and OCT imaging can help monitor for complications such as retinal detachment or residual inflammation.
This structured approach, from vitrectomy to careful cyst removal, aims to achieve optimal outcomes when managing intraocular cysticercosis and preserving vision. RS



