Take-home points
|
 |
Bios Dr. Masaki Fukushima is a vitreoretinal surgeon at Kindai University and the University of Toyama, Japan. Dr. Akihiko Shiraki is a vitreoretinal surgeon at Osaka University, Japan. Dr. Taku Wakabayashi is a vitreoretinal surgeon at Wakabayashi Eye Center and a clinical professor of ophthalmology at Kanazawa University, Japan. Disclosures: The authors have no relevant financial disclosures. |
The prevalence of high myopia is rising worldwide, predicted to increase by nearly 9.8 percent (approximately 1 billion people) globally by 2050.1 This trend suggests that the vision-threatening complications associated with high myopia, including macular hole retinal detachment, will become increasingly important.
MHRD is a retinal detachment associated with a full-thickness macular hole. It occurs predominantly in highly myopic eyes with posterior staphyloma, but its pathogenesis differs from that of primary rhegmatogenous RD associated with concurrent MH in non-highly myopic eyes. The pathogenesis of MHRD is multifactorial, involving tangential traction from the vitreous cortex and epiretinal membrane,2 anteroposterior traction associated with posterior staphyloma3 and reduced adhesion between the retina and retinal pigment epithelium due to myopic maculopathy (chorioretinal atrophy).3 Both tangential and anteroposterior traction promote MH formation, which is followed by the entry of subretinal fluid through the hole and progression to MHRD. Because these tractional forces constitute the underlying pathology, the goals of surgery are to relieve this traction, achieve MH closure and reattach the retina.
Our surgical techniques
Here are our strategies and important considerations for each step of MHRD repair:
• Incision. We perform pars plana vitrectomy with an inverted ILM flap and long-acting gas tamponade as our first-line technique for MHRD (see video below). In highly myopic eyes, standard sclerotomy sites (3.5 to 4 mm) may not allow forceps to reach the macula because of the long axial length. The distance from the limbus to the ora serrata is greater in highly myopic eyes than in non-myopic eyes and commonly exceeds 5 mm in eyes with an axial length over 27 mm.4 Therefore, creating sclerotomies more posteriorly (approximately 5 mm from the limbus) helps in reaching the macula.
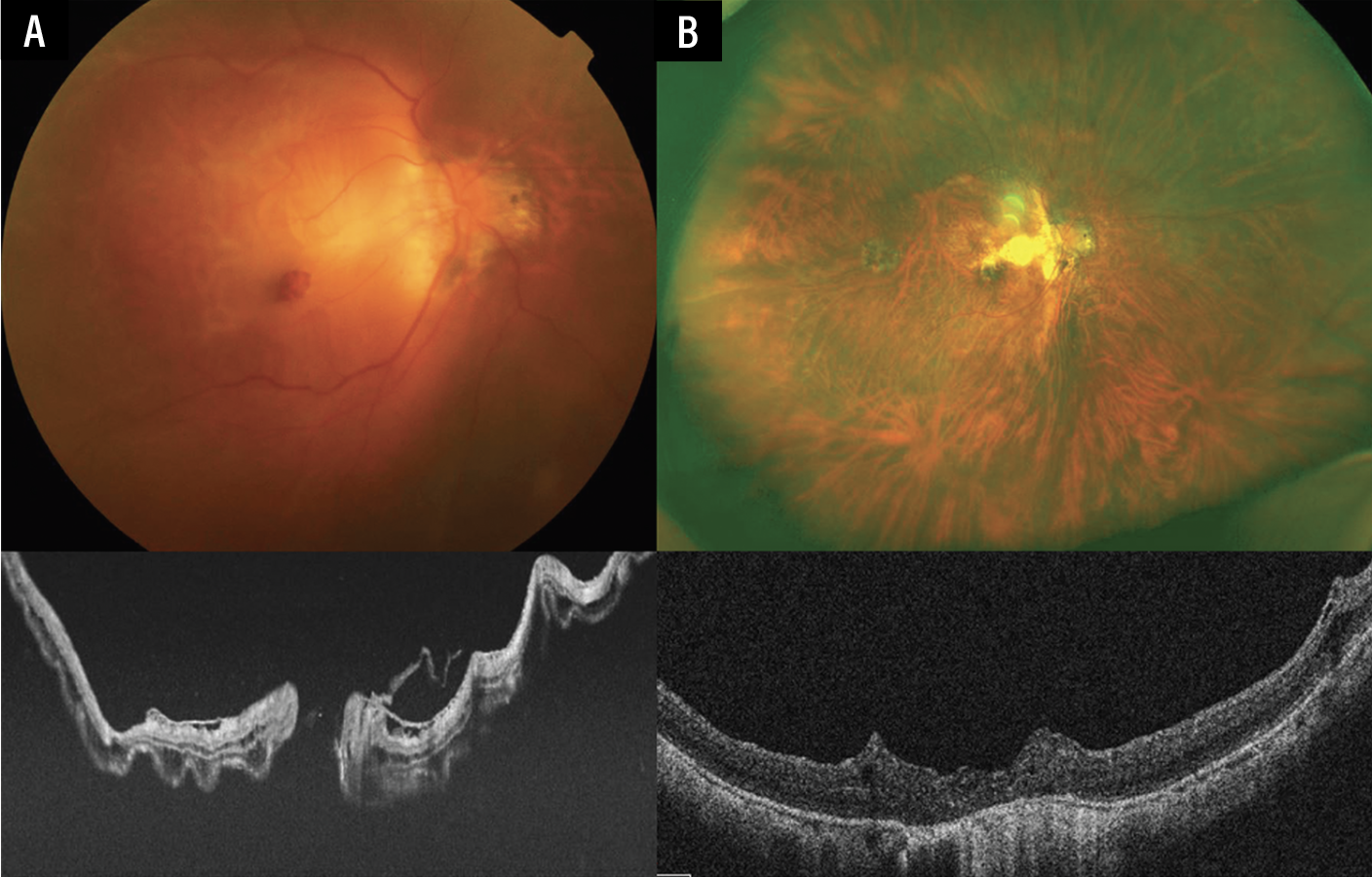 |
| Figure 1. Preoperative and postoperative images of a patient with macular hole retinal detachment in a highly myopic eye. (A) Preoperative fundus photograph and OCT show MHRD. The axial length was 30.9 mm. (B) Postoperative images demonstrate successful macular hole closure and retinal reattachment after vitrectomy, ILM flap and 10 percent C3F8 tamponade. The vision improved from 20/1000 to 20/100. |
Another helpful technique is to first create a standard sclerotomy on the nondominant (e.g., left hand) side and then insert the light pipe into the vitreous cavity to identify the ora serrata on the dominant (e.g., right hand) side by observing transillumination from within the eye. Because the retina and pars plana differ in their light-transmission characteristics, the boundary between them can be clearly distinguished (see video below). Direct visualization of the ora serrata with scleral indentation is another useful technique for safe entry.
• Long-shafted instruments. Preoperative measurement of the axial length is useful for determining whether standard forceps will suffice or long-shafted instruments are required. In eyes with an axial length greater than 32 mm, long-shafted forceps may be an option. Alternative approaches include temporarily lowering the infusion pressure or removing the cannula to gain further distance.
• Vitreous cortex removal. Since the vitreous plays a key role in the pathogenesis of MHRD,5 complete separation of the posterior hyaloid and removal of vitreous cortex remnants and ERMs are essential for successful retinal reattachment. As first described by Drs. Stirpe and Michels,2 even in eyes with posterior vitreous detachment, vitreoschisis very commonly occurs in highly myopic eyes, often leaving residual vitreous cortex remnants and ERMs adhered to the posterior pole and beyond. Triamcinolone acetonide should be used routinely to assess the status of PVD and visualize the vitreous cortex remnants and ERMs. Repeated triamcinolone staining, combined with the use of forceps, a diamond-dusted membrane scraper (Tano scraper, Bausch + Lomb) or a Finesse Flex Loop (Alcon), facilitates the efficient removal of the vitreous cortex from the posterior pole.
In eyes with a highly elevated detached retina, these maneuvers can be challenging. In such cases, drainage of subretinal fluid through the preexisting MH may help flatten the retina and improve manipulation. However, SRF should be gently aspirated, as active drainage may enlarge the MH and cause additional foveal damage.
• Internal limiting membrane staining and flap. Complete removal of the multilayered vitreous cortex improves subsequent ILM staining with Brilliant Blue G and indocyanine green. After we stain the ILM, we create a multilayer inverted ILM flap to cover the hole. Since hole closure rates are around 40 percent after conventional complete ILM peeling, we routinely use an ILM flap to improve the hole closure. A multilayer flap provides more reliable coverage than a single-layer flap, particularly in large MHs. Viscoelastic is a useful material for stabilizing the inverted flap over the hole. The remaining ILM not used for the flap is broadly peeled, ideally extending from arcade to arcade.
Whether the ILM flap should be covered or inserted into the hole remains controversial. We use the cover technique for small-to-medium-sized holes that show less extensive SRF. However, flap displacement may occasionally occur during fluid-air exchange or in the postoperative period, resulting in persistent macular hole opening. For this reason, an insertion technique is often preferred, especially in large MHs and cases with extensive SRF, as this provides greater flap stability, even during fluid-air exchange.6 The potential disadvantage of an insertion technique is the formation of a glial scar at the fovea; however, hole closure is prioritized in cases with MHRD caused by large MH.
Several technical approaches can be considered when creating ILM flaps in eyes with MHRD. The inverted ILM flap can be performed under fluid without the use of perfluorocarbon liquid. In cases of MHRD within the posterior pole, SRF drainage is unnecessary when performing ILM flaps. In eyes with highly elevated detached retinas, gentle aspiration of SRF through the hole reduces the retinal height and aids in flap manipulation. Avoiding PFCL allows easier forceps access to the macula, as the detached retina rises anteriorly and shortens the working distance; however, flap stability may be reduced. Therefore, PFCL can be used to flatten the retina and provide better control when positioning the inverted ILM flap. In cases of inadequate ILM staining, restaining with the dye under PFCL can also be effective (see video below). The potential disadvantage of using PFCL is the increased distance between the sclerotomy site and the macula, although long-shafted forceps can overcome this limitation.
• Fluid-air exchange. After peripheral vitreous shaving, we perform fluid-air exchange. During this exchange, the SRF can usually be left in place, especially when the RD is limited to the posterior pole or can be drained through a drainage retinotomy that’s created outside the vascular arcade in cases of extensive RD. The SRF can also be aspirated through the original MH; however, this carries the risk of hole enlargement and may cause RPE damage from the soft-tip cannula. Therefore, we don’t recommend complete SRF aspiration through the MH. Successful retinal reattachment can be achieved even without complete fluid removal.
• Tamponade. The most commonly used long-acting gas tamponades include 20 percent SF6 or 10 percent C3F8 gas, with one study showing comparable outcomes between the two.7 Another study reported higher retinal reattachment rates with gas compared with silicone oil, although the MH closure rates and final visual acuity didn’t differ significantly between the two groups.8 Nevertheless, silicone oil tamponade remains an effective option, especially in only one seeing eye (relatively common in severe pathologic myopia) or in cases of recurrence or proliferative vitreoretinopathy that require prolonged tamponade.
• Macular buckle and other techniques. Although most MHRDs can be successfully managed with PPV alone, recurrent MHRD may require alternative techniques, such as human amniotic membrane transplantation or autologous retinal transplantation.9,10 In some cases, macular buckle is also effective for recurrent MHRD despite prior vitrectomy with ILM peeling and tamponade, as the procedure relieves anteroposterior traction by indenting the posterior pole and counteracting the deforming forces of the posterior staphyloma.11,12
Surgical outcomes
A recent meta-analysis indicates that hole closure rates are around 40 percent after vitrectomy with complete ILM peeling, 94.3 percent with the ILM flap covering and 91.6 percent with the ILM flap insertion technique.13 The reattachment rates are 69 percent to 100 percent after complete ILM peeling, 91.8 percent after ILM flap covering and 97.1 percent after the ILM flap insertion.13 The hole closure is an important factor for retinal reattachment, and using an ILM flap increases the likelihood of positive anatomic outcomes. Visual improvement can be achieved in more than 80 percent of eyes treated with the inverted ILM flap.13 However, the mean visual acuity after vitrectomy is often lower than 20/200.14 A longer axial length is generally a poor prognostic factor.
Recurrent RD and PVR are major postoperative complications after vitrectomy for MHRD. Identification and removal of residual vitreous cortex, ERMs and any remaining ILM are critical during reoperation. However, the cause of redetachment is sometimes difficult to identify. In those cases, the responsible factors may be persistent traction due to posterior staphyloma and underlying severe chorioretinal atrophy. For cases with these issues, surgeons may consider alternatives, such as macular buckle, human amniotic membrane transplantation and autologous retinal transplantation.
Rhegmatogenous RD with concurrent MH
In primary RRD with concurrent MH in non-highly myopic eyes, the detachment is caused by peripheral retinal breaks, whereas the MH is a coexisting rather than causative lesion (Figure 2). Surgical management includes PPV, peripheral vitreous shaving and intraocular tamponade. ILM peeling may be performed to facilitate MH closure; however, an inverted ILM flap may also be considered in large MHs. Anatomic outcomes are similar between RRD with and without concurrent MH; however, visual outcomes are worse in eyes with concurrent MH.15
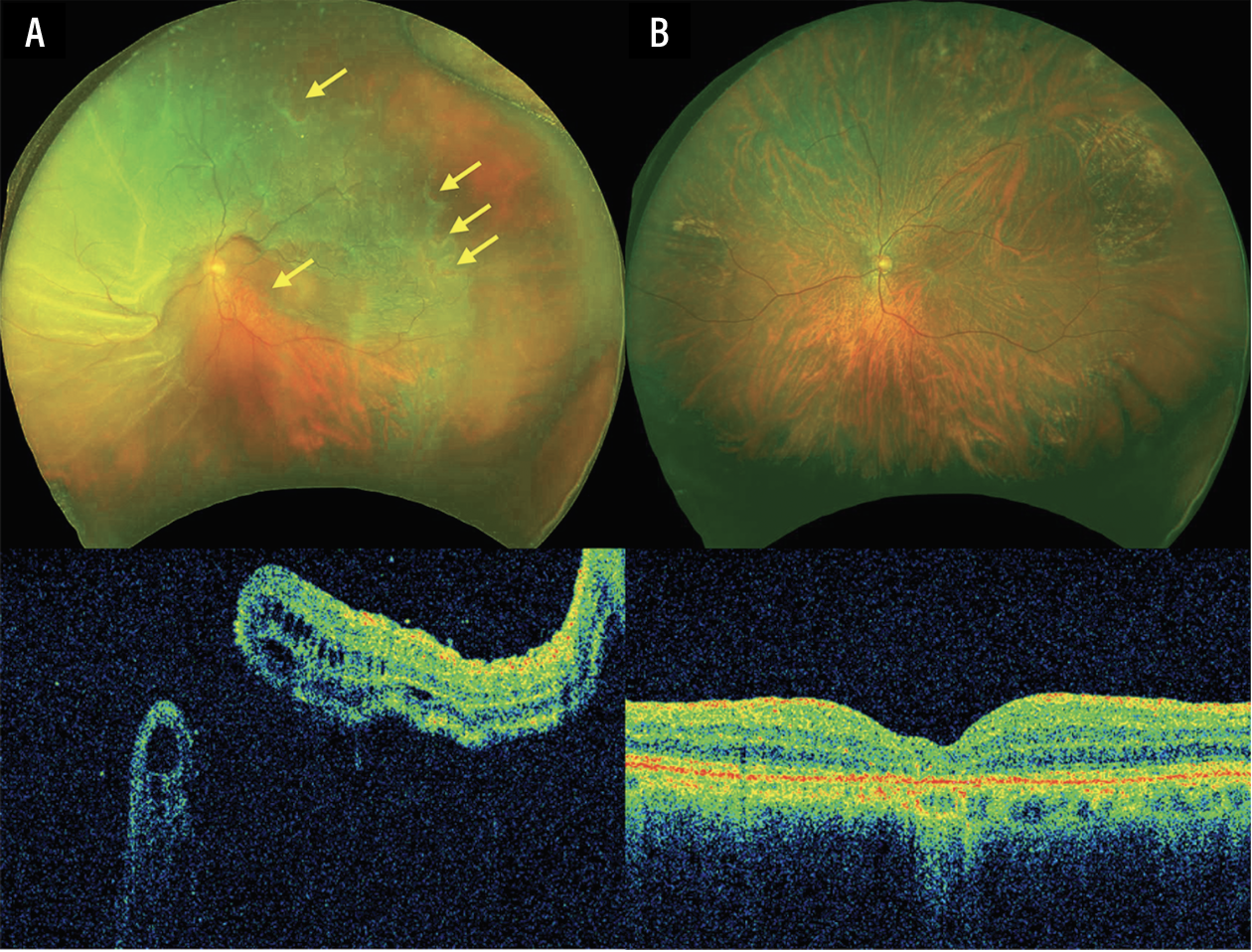 |
| Figure 2. Preoperative and postoperative images of a patient with primary rhegmatogenous retinal detachment and concurrent macular hole a in non-highly myopic eye. (A) Preoperative fundus photograph and OCT show multiple peripheral breaks and concurrent macular hole (yellow arrows). The axial length was 24.5 mm. (B) Postoperative images demonstrate successful macular hole closure and retinal reattachment after vitrectomy, ILM peeling and 20 percent SF6 gas tamponade. The vision improved from 20/1000 to 20/200. |
Conclusion
PPV, ILM flap and long-acting gas tamponade are the mainstays of treatment for MHRD in highly myopic eyes. However, surgical techniques should be individualized, as the MH size, extent of RD, severity of myopic maculopathy and presence or absence of PVR may vary in each case, resulting in varied surgical approaches. A thorough understanding of the underlying pathologies and optimal surgical techniques is essential for improving long-term anatomic and visual outcomes in this challenging condition. RS
REFERENCES
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 2016;123:5:1036-1042.
2. Stirpe M, Michels RG. Retinal detachment in highly myopic eyes due to macular holes and epiretinal traction. Retina 1990;10:2:113-114.
3. Morita H, Ideta H, Ito K, et al. Causative factors of retinal detachment in macular holes. Retina 1991;11:3:281-284.
4. Hirono K, Inoue M, Tanaka S, et al. Anterior segment optical coherence tomography in determination of entry site for vitrectomy in highly myopic eyes. Retina 2023;43:5:733-738.
5. Gonvers M, Machemer R. A new approach to treating retinal detachment with macular hole. Am J Ophthalmol 1982;94:4:468-472.
6. Chen SN, Yang CM. Inverted internal limiting membrane insertion for macular hole-associated retinal detachment in high myopia. Am J Ophthalmol 2016;162:99-106.e1.
7. Nakanishi H, Kuriyama S, Saito I, et al. Prognostic factor analysis in pars plana vitrectomy for retinal detachment attributable to macular hole in high myopia: A multicenter study. Am J Ophthalmol 2008;146:2:198-204.
8. Kakinoki M, Araki T, Iwasaki M, et al. Surgical outcomes of vitrectomy for macular hole retinal detachment in highly myopic eyes a multicenter study. Ophthalmol Retina 2019;3:10:874-878.
9. Caporossi T, Angelis LD, Pacini B, et al. A human amniotic membrane plug to manage high myopic macular hole associated with retinal detachment. Acta Ophthalmol 2020;98:2:e252-256.
10. Moysidis SN, Koulisis N, Adrean SD, et al. Autologous retinal transplantation for primary and refractory macular holes and macular hole retinal detachments—The Global Consortium. Ophthalmology 2021;128:5:672-685.
11. Ge JY, Teo AWJ, Tsai ASH, et al. Macular buckle, vitrectomy or combined approach for the management of macular hole retinal detachment: A systematic review and network meta-analysis. Ophthalmol Retina 2025; doi:10.1016/j.oret.2025.08.020.
12. Ripandelli G, Coppé AM, Fedeli R, et al. Evaluation of primary surgical procedures for retinal detachment with macular hole in highly myopic eyes: A randomized comparison of vitrectomy versus posterior episcleral buckling surgery. Ophthalmology 2001;108:12:2258-2264.
13. Chatziralli I, Machairoudia G, Kazantzis D, Theodossiadis G, Theodossiadis P. Inverted internal limiting membrane flap technique for myopic macular hole: A meta-analysis. Surv Ophthalmol 2021;66:5:771-780.
14. Wakabayashi T, Ikuno Y, Shiraki N, et al. Inverted internal limiting membrane insertion versus standard internal limiting membrane peeling for macular hole retinal detachment in high myopia: One-year study. Graefes Arch Clin Exp Ophthalmol 2018;256:8:1387-1393.
15. Starr MR, Obeid A, Ryan EH, et al. Surgical outcomes of primary RRD with and without concurrent full-thickness macular hole (PRO Study Report No. 7). Ophthalmic Surg Lasers Imaging Retina 2020;51:9:500-505.



