
|
Bios Dr. Uner is a uveitis fellow at Casey Eye Institute, Oregon Health & Science University in Portland, Ore., and is an incoming vitreoretinal surgery fellow at Tennessee Retina in Nashville, Tenn. Dr. Suhler is professor of ophthalmology and public health at Oregon Health & Science University, director of the uveitis division and uveitis fellowship at Casey Eye Institute, and chief of ophthalmology at VA Portland Health Care System, all in Portland. Disclosures: Dr. Suhler receives research support from Merck, Priovant, Regeneron, Roche/Genentech, and is a consultant for Roche/Genentech, all unrelated to this work. He is supported by the Department of Veterans Affairs. Both authors are supported by an unrestricted grant to the Casey Eye Institute from Research to Prevent Blindness to the Casey Eye Institute. |
Retinal vasculitis is a presentation of uveitis that can be intimidating to the physician and devastating for the patient. Here, we provide a framework for effective diagnosis, management and treatment of the inflammatory and infectious drivers of this condition.
Definition and presentation
Retinal vasculitis is defined as inflammation of retinal arterioles, venules and/or capillaries. Per the Standardization of Uveitis Nomenclature Working Group, the term is used in cases with evidence of ocular inflammation and retinal vascular changes.1 These changes may include sheathing, perivascular cuffing, hemorrhage and exudation in non-occlusive cases, and vascular occlusion with cotton wool spots or patches of inner retinal whitening, pre-retinal or intraretinal hemorrhages, and retinal neovascularization in occlusive cases.2 Retinal vasculitis can be primary, or secondary to identifiable ocular or systemic inflammatory diseases.
Involved vessels may be retinal veins (phlebitis), arteries (arteriolitis) or capillaries (capillaritis). Patients can be asymptomatic or present to the clinic with blurred vision, flashes, floaters, scotomas and/or metamorphopsia. Color vision changes can be seen if the optic nerve or macula are involved. Pain can also be a presenting symptom, either related to concurrent intraocular inflammation or ocular ischemia.2
Multimodal imaging
Retinal imaging is crucial in the diagnosis and follow-up of retinal vasculitis. It’s not uncommon to find patches of vascular sheathing in the periphery of a patient with non-specific complaints on widefield fundus imaging, clinching the diagnosis.
Serial fundus photography is important and may demonstrate changes in the retina and/or vasculature over time. Fundus autofluorescence may be unremarkable despite active vasculitis or show hyperautofluorescence corresponding to areas of stressed retinal pigment epithelium from ischemia. Hypoautofluorescence can be seen in areas of blocked AF from hemorrhage or atrophic RPE. Over time, despite treatment, hypoautofluorescent lesions can be seen along retinal vessels, indicating RPE migration and changes related to chronic inflammation.3
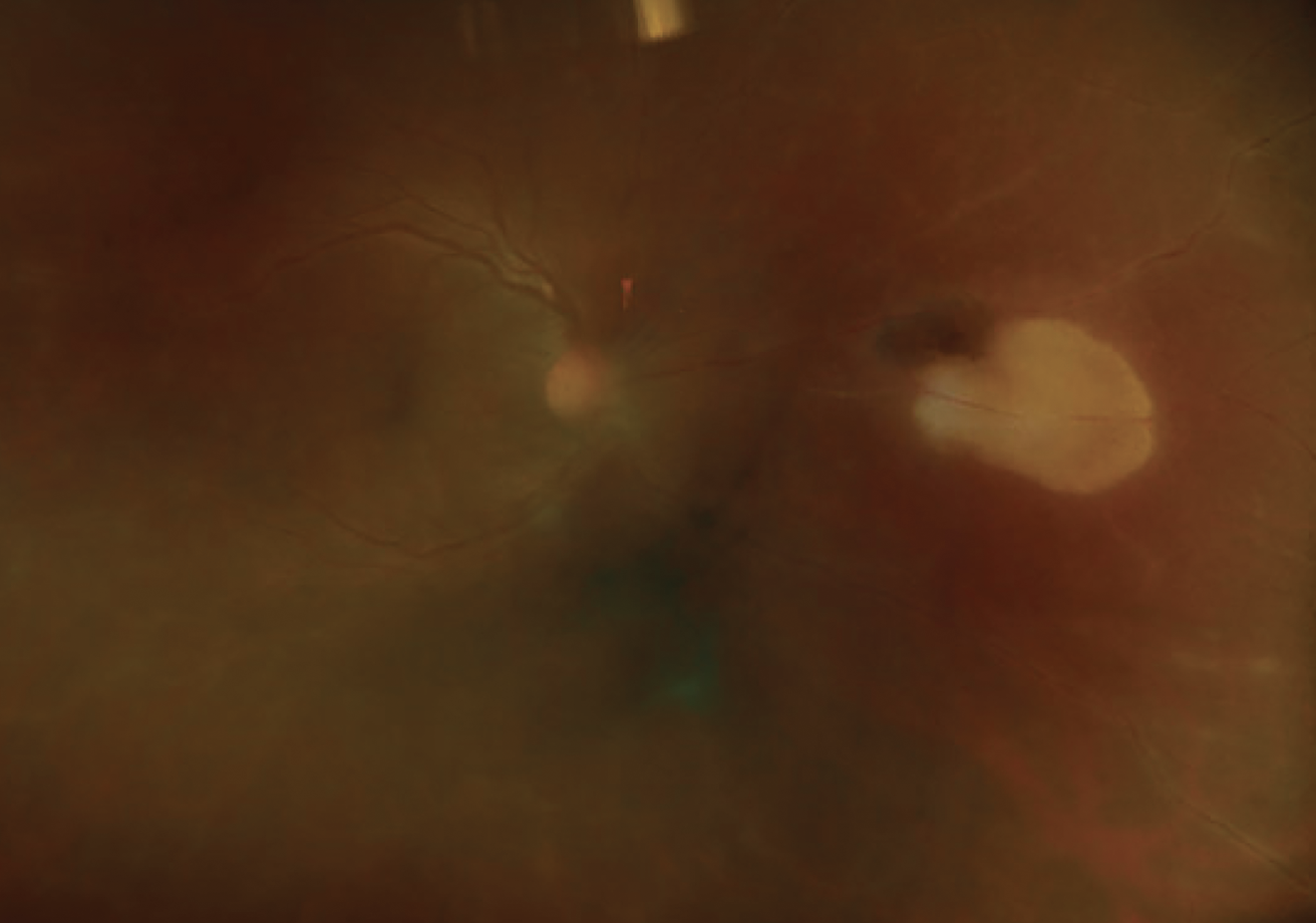 |
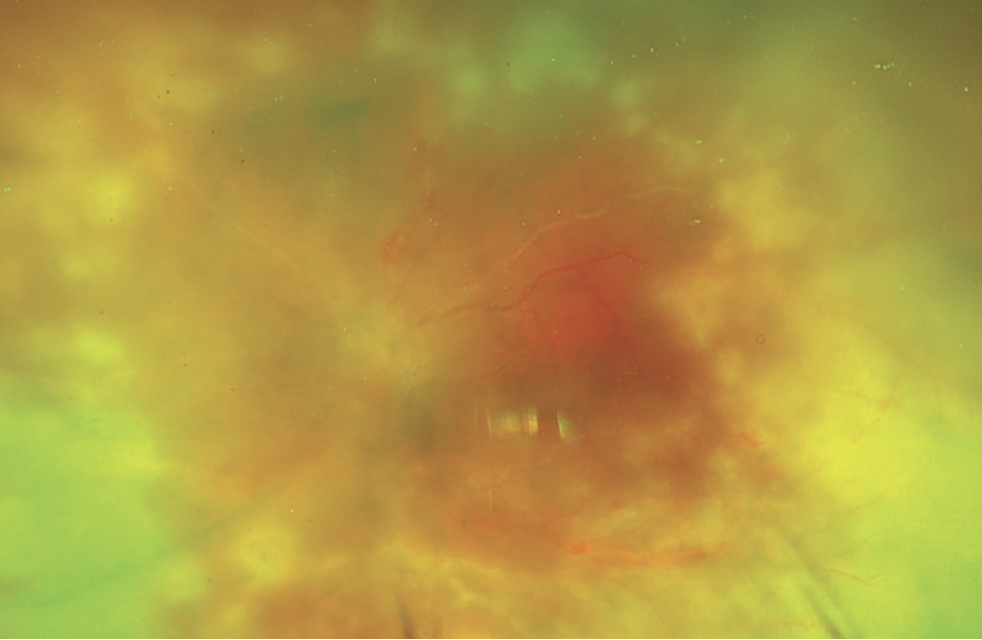
| Figure 1. Predominant phlebitis in toxoplasmosis. |
Fluorescein angiography is the gold standard of the diagnosis of retinal vasculitis, showing vessel leakage and staining of blood vessel walls in active disease. Leakage is due to inflammation and subsequent breakdown of the blood-retina barrier and may persist even after inflammation control, so it’s important to note that not every leaking vessel indicates active disease. Conversely, angiography may reveal significant active leakage in patients with a relatively normal retinal exam; hence, we believe every patient with intermediate uveitis or recurrent cystoid macular edema should have an FA even in the absence of vascular sheathing on clinical examination. The leakage can be diffuse, as commonly seen in Behçet’s disease, or segmental, as in sarcoidosis and multiple sclerosis.2 Other findings often seen include petaloid leakage in cystoid macular edema, optic disc leakage or staining, retinal ischemia, occlusions or nonperfusion and neovascularization of the disc and elsewhere. Behçet’s disease and pars planitis may be accompanied by diffuse fern-like capillary leakage, which is a poor prognostic sign, predicting likely the need for aggressive immunomodulatory therapy.
 |
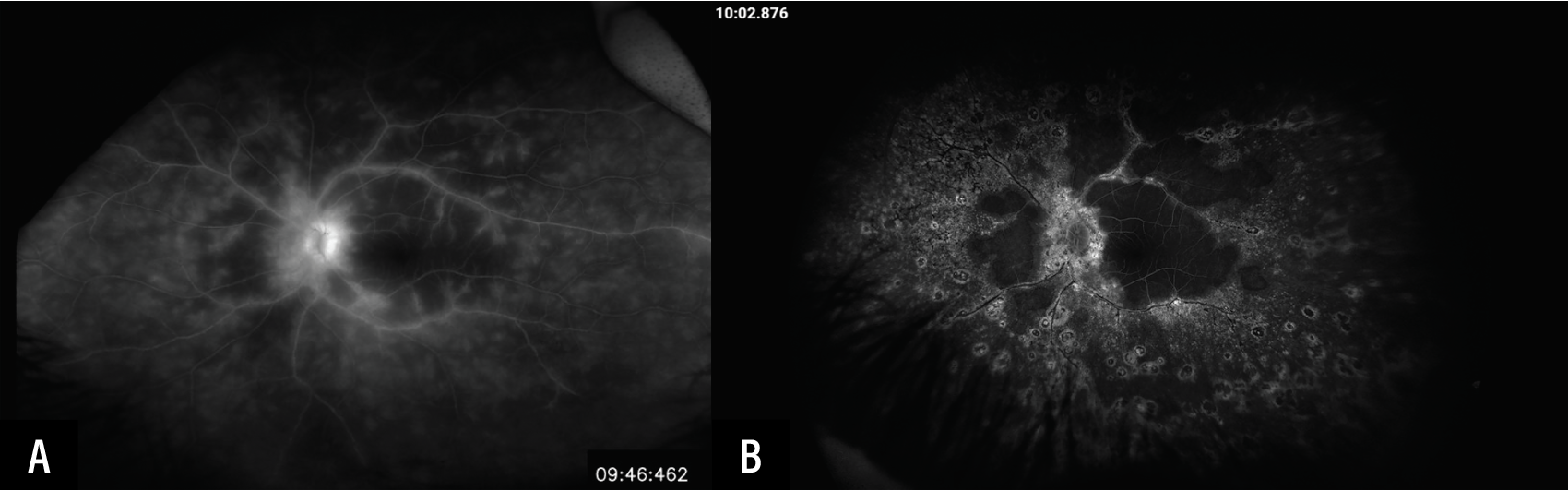
| Figure 2. Non-occlusive phlebitis in pars planitis (A) with leakage on fluorescein angiography (B). |
Peripheral retinal vascular pruning and remodeling on FA can be seen in cases of Zone 2 and 3 non-occlusive retinal vasculitis. Given physiologic variability in peripheral avascular zones, these cases shouldn’t be classified as occlusive disease unless there are clear angiographic or clinical signs of retinal non-perfusion, such as discrete areas of capillary dropout, terminal vessel truncation or vascular amputation rather than gradual attenuation, persistent capillary voids extending beyond expected physiologic peripheral avascular retina for age and refractive status, associated ischemic sequalae and/or correlations with structural changes, such as inner retinal thinning on widefield OCT.
Optical coherence tomography will show various macular edema subtypes and can distinguish this from serous retinal detachment. Visual acuity often correlates with the presence of macular edema. Perivascular retinal thickening and subfoveal choroidal thickness can also serve as OCT biomarkers and have been demonstrated to be useful biomarkers of response to corticosteroid treatment in birdshot choroidopathy.4 Other reports have shown a positive correlation between subfoveal choroidal thickness and total retinal leakage score in several non-infectious etiologies of retinal vasculitis, with a study showing subjective complaints in birdshot chorioretinopathy were associated with suprachoroidal fluid on enhanced depth imaging-OCT.5,6 Obtaining EDI-OCT for these measures is especially useful in uveitis patients with suspected retinal vasculitis in settings where access to FA is limited.
OCT angiography is becoming ubiquitous in retina clinics and can be helpful in the identification of complications associated with retinal vasculitis, such as capillary dropout, enlarged foveal avascular zone, telangiectasias, shunt vessels and neovascularization. Some studies have reported retinal capillary vessel density alterations, whereas others haven’t been able to conclusively show signs of active inflammation around affected vessels on OCTA despite leakage on FA.5,7 Widefield OCTA may be used to evaluate for peripheral non-perfusion, collateral vessel formation and neovascularization.8 Further studies on standard and widefield OCTA are needed to compare its applicability to FA, and make it more generalizable in the evaluation of retinal vasculitis.
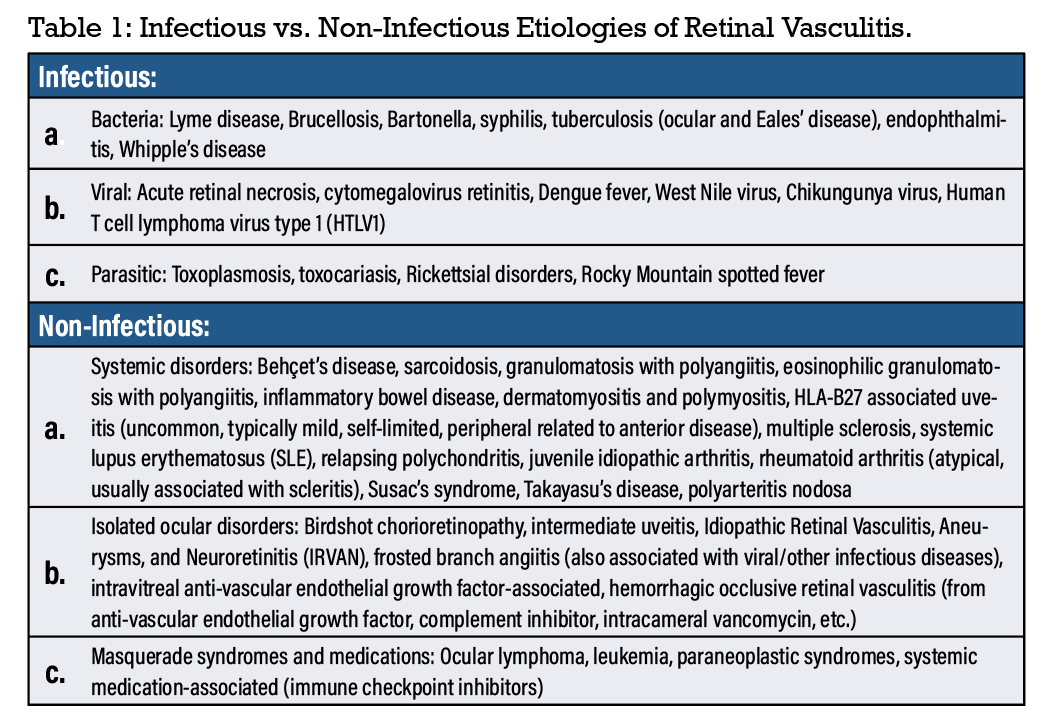 |
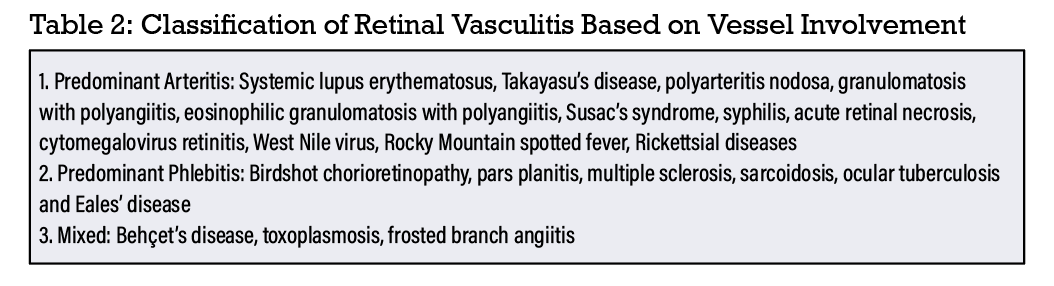
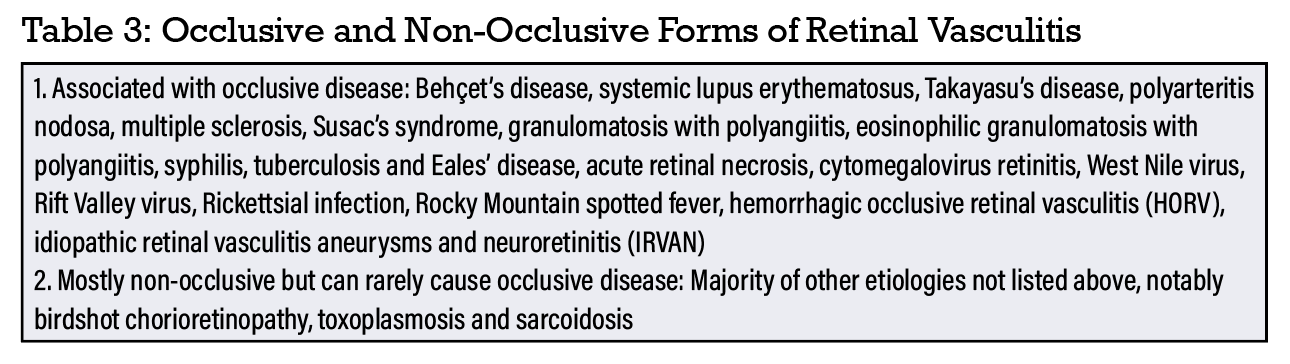
Etiologies
There is no established classification of retinal vasculitis, but it has historically been classified based on etiology (infectious or non-infectious), vessels involved (predominant arteritis or phlebitis) and presence of inflammatory vessel occlusion (occlusive or non-occlusive). For this article, we present these three frameworks consisting of overlapping etiologies that can help narrow down the differential diagnosis (Tables 1-3). It’s important to note that some non-occlusive etiologies can become occlusive over time without treatment. Similarly, those that present with arteritis can involve venules without treatment. Intravitreal anti-VEGF or complement inhibitor therapies can cause isolated retinal vasculitis, which can be hemorrhagic or non-hemorrhagic.
A general work-up consists of evaluation for syphilis (treponemal followed by non-treponemal testing), tuberculosis (interferon-gamma release assay preferred, but can also do PPD skin testing), sarcoidosis (chest imaging, ACE/lysozyme in suspicious cases) and systemic vasculitides (at a minimum CBC, CMP and an ANCA panel) in all patients, as well as a more targeted work-up (e.g., MRI brain to evaluate for multiple sclerosis) for other etiologies based on review of systems, demographic information, risk factors and presence of intraocular inflammation elsewhere in the eye(s).
 |
 |
A meta-analysis published in Survey of Ophthalmology in 2025 as part of The International Uveitis Study Group’s Retinal Vasculitis Study (ReViSe) project, studied 8,149 patients with retinal vasculitis.9 It concluded that over half of the cases were secondary to infectious or non-infectious diseases, with the most common etiologies being Behçet’s disease, sarcoidosis, tuberculosis and toxoplasmosis. Idiopathic cases comprised 38 percent of all patients with retinal vasculitis, and 8 percent had retinal vasculitis with concomitant inflammation of non-retinal ocular structures.9 This underscores the importance of a thorough review of systems and systemic work-up in patients with retinal vasculitis.
Treatment principles
 |
| Figure 3. Occlusive retinal arteritis in a patient with acute retinal necrosis. |
Most cases of retinal vasculitis require treatment to prevent irreversible retinal damage and reduce the risk of macular edema. FA can be helpful in delineating the extent of the vasculitis and guide treatment. In general, observation is appropriate for leakage beyond Zone 3 of the posterior segment, if minimal and stable. A study on patients with peripheral vascular leakage showed this finding doesn’t confer an increased risk of impaired vision or cystoid macular edema after more than a year of follow-up.10 This study also found that peripheral leakage was an independent driver of clinical treatment escalation. Hence, a careful evaluation of visual and other imaging findings is necessary to avoid overtreatment based solely on leakage. As mentioned previously, not every area of leakage on FA is indicative of active disease, so a high-dose prednisone challenge (e.g., prednisone 1 mg/kg/day daily for one to two weeks with a follow-up FA) can be considered to determine if it represents active disease. Occlusive retinal vasculitis always requires treatment to prevent its several complications. Retinal vasculitis associated with systemic diseases, especially Behçet’s disease and ANCA-associated vasculitides, requires concomitant treatment of ocular and systemic manifestations. Unlike some systemic vasculitis that can sometimes be treated with nonsteroidal anti-inflammatory agents, retinal vasculitis requires more aggressive management.
 |
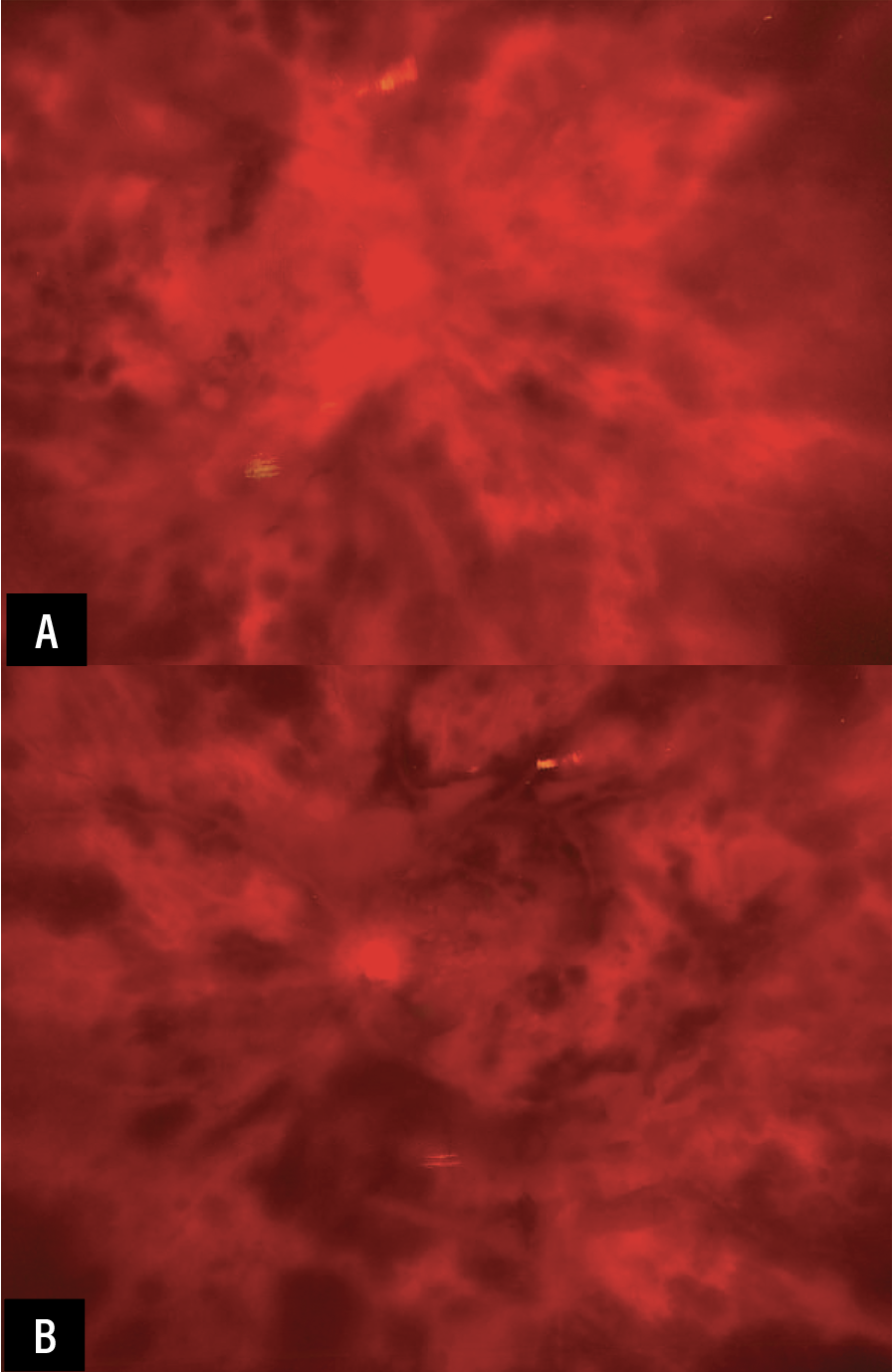
| Figure 4. Diffuse fern-like leakage in a young patient with granulomatous panuveitis with non-occlusive retinal vasculitis before (A) and 12 years later (B), with incomplete response to infliximab, adalimumab, cyclosporine, mycophenolate, methotrexate, tocilizumab and subcutaneous interferon alfa-2a and final achievement of quiescence with an intravitreal fluocinolone acetonide 0.19 mg implant. Note significant retinal atrophy at final follow-up due to vasculitis. |
Isolated peripheral (mostly Zone 3, sometimes bordering Zone 2) leakage is common after pars plana vitrectomy in patients, often with old pigmented vitreous cell. Unless accompanied by other signs of active ocular inflammation (e.g., anterior chamber cell, vitreous haze) or inflammatory sequelae such as macular edema, this leakage doesn’t require treatment. Observation with exams every two to three months is a reasonable initial approach for these cases.
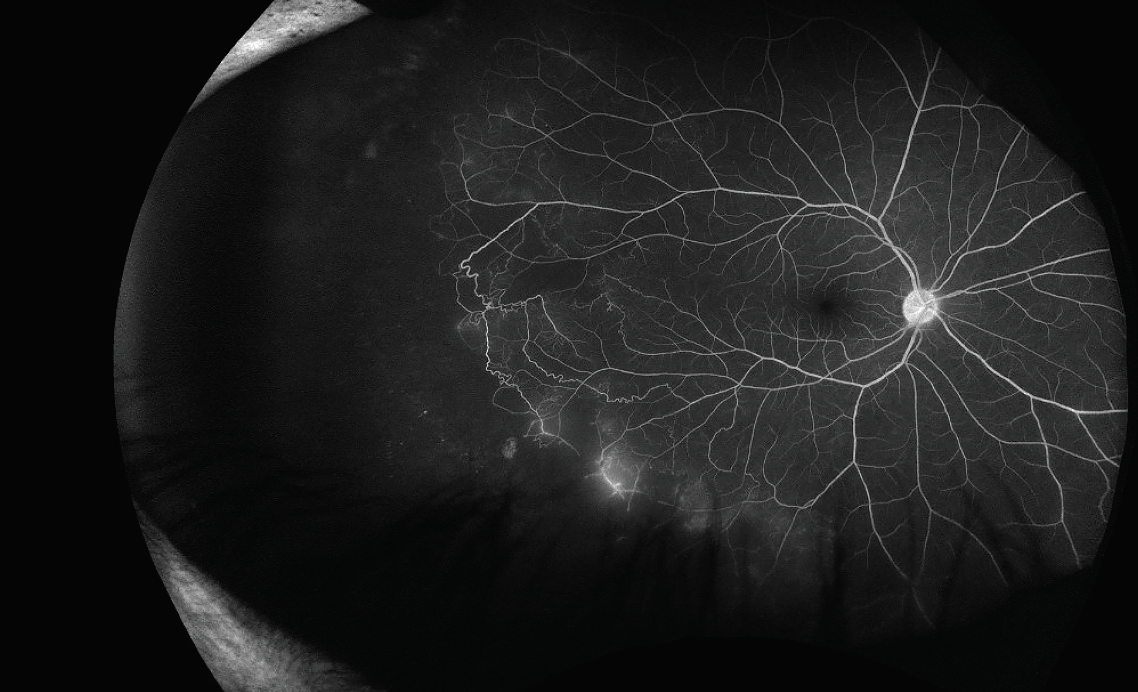 |
| Figure 5. Peripheral occlusive vasculitis in a patient diagnosed with Eales’ disease after positive Quantiferon testing. |
Topical treatment has little or no role in the treatment of primary or systemic disease-associated retinal vasculitis, as it doesn’t meaningfully penetrate to the posterior segment. However, topical difluprednate may be useful adjunctive treatment of macular edema and mild peripheral leakage when deemed secondary to anterior segment or vitreous inflammation.
The mainstay of treatment of Zones 1 and 2 retinal vasculitis, with or without macular edema, is systemic corticosteroids, dosed at 60 mg daily or 1 mg/kg/day (whichever is lesser) and gradually tapered in conjunction with systemic immunomodulatory therapy (IMT), such as methotrexate, mycophenolate, azathioprine, tumor necrosis factor-alpha blockers such as adalimumab and infliximab, interleukin-6 receptor blockers such as tocilizumab, or B-cell depleting agents such as rituximab. Tocilizumab has great efficacy in the treatment of uveitic macular edema and has been used successfully in retinal vasculitis. A retrospective study of 35 eyes showed that infliximab and tocilizumab were similarly effective in improving vascular leakage and central subfield thickness in patients with non-infectious retinal vasculitis over six months.11
 |
| Figures 6A-B. Diffuse bilateral occlusive retinal vasculitis after bilateral same-day intravitreal pegcetacoplan injections for GA. |
Local corticosteroids remain a good acute treatment option for pseudophakic patients, as well as for those with unilateral disease or who aren’t good candidates for systemic immunosuppression, or as a bridge to appropriate therapy while immunosuppression is taking effect. Intravitreal dexamethasone 0.7 mg implant (Ozurdex, AbbVie, Irvine, California) and 0.05 to 0.1mL intravitreal triamcinolone 40 mg/mL (Triescence, Harrow, Nashville, Tennessee.) last approximately three months and are often combined with IMT for long-term management. Periocular corticosteroid injections of triamcinolone are a well-established option, which have been shown to be less effective than intravitreal steroids but are less likely to elevate intraocular pressure. Intravitreal fluocinolone acetonide implant 0.19 mg (Iluvien, Alimera Sciences, Alpharetta, Georgia), which lasts up to 36 months, may be another long-term option for patients who can’t be on IMT and to reduce the need for serial intravitreal or periocular injections.
Managing complications
Untreated non-occlusive retinal vasculitis can lead to macular edema and retinal degeneration. If left untreated, occlusive vasculitis can be even more visually devastating, progressing to complications such as vitreous hemorrhage, tractional and rhegmatogenous retinal detachments, and neovascular glaucoma.
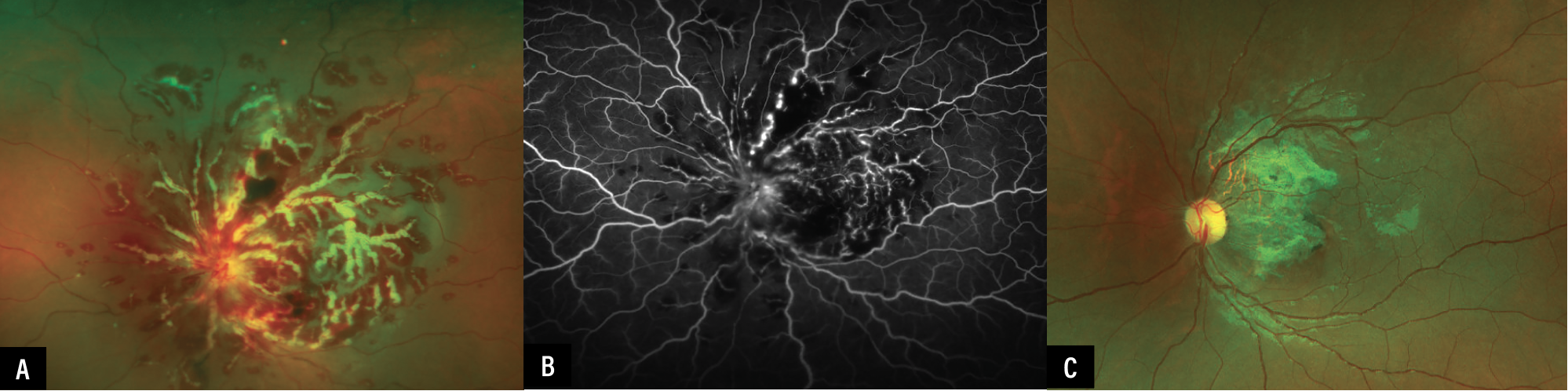 |
| Figure 7. Occlusive retinal vasculitis with a frosted branch angiitis appearance in a patient with ANCA-associated vasculitis (A). Note FA with areas of hypofluorescence from vascular occlusion, as well as leakage from perfused vessels and the disc (B). After treatment with prednisone and rituximab, the previously inflamed areas are left with fibrosis and vascular attenuation (C). |
Anti-VEGF injections are effective for the treatment of NV secondary to retinal vasculitis. However, control of the underlying infectious or inflammatory disease is paramount. Sectoral or panretinal photocoagulation to areas of ischemia can be performed to reduce the likelihood of recurrent NV and tractional sequelae when the inflammation is well-controlled.12 Though no clear guideline exists on the duration of quiescence, a three-month period of inactivity on FA similar to other intraocular procedures is reasonable. Cryotherapy has also been used to treat retinal vasculitis associated with pars planitis.13
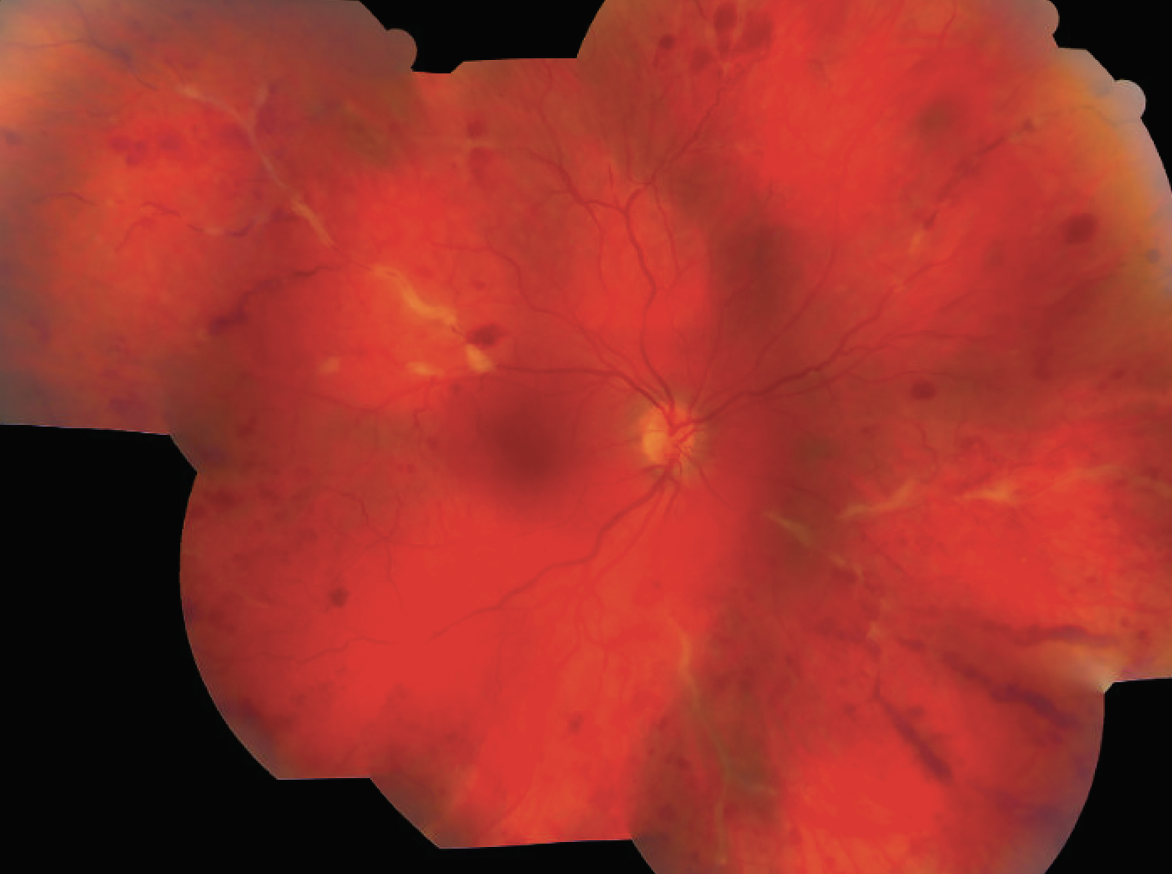 |
| Figure 8. Widespread retinal venulitis with hemorrhages in a patient with sarcoidosis. |
Pars plana vitrectomy is indicated for non-clearing vitreous hemorrhage, retinal detachment or concern for masquerade syndromes, such as vitreoretinal lymphoma. In cases of non-infectious and non-neoplastic retinal vasculitis, peri-operative inflammatory control is essential. We advise initiation of systemic prednisone 1 mg/kg/day three days prior to surgery and intravenous methylprednisolone 125 mg intraoperatively, followed by a prednisone taper over at least a month. Intraoperative posterior Sub-Tenon’s triamcinolone acetonide (Kenalog, Bristol-Myers-Squibb, Canada), Ozurdex or anti-VEGF can also be considered on a case-by-case basis. If there is diagnostic uncertainty or concern for a masquerade syndrome, we recommend steroid avoidance or discontinuation at least two weeks prior to vitrectomy to maximize diagnostic yield.
When to refer to a uveitis specialist
Most cases of retinal vasculitis should be referred to a uveitis specialist for consideration of IMT. Urgent referral (in one to two days if able) is indicated in occlusive disease for early IMT initiation. If there is suspicion for infectious vasculitis, the treating specialist should perform an anterior chamber or vitreous tap and injection of antimicrobials with broad coverage and assess need for referral based on clinical response. Bilateral or severe intraocular inflammation accompanying the retinal vasculitis requires prompt referral (within one to two weeks). Recurrent disease despite initial corticosteroid treatment and cases that require chronic oral prednisone >7.5 mg/kg/day should also be referred expeditiously.
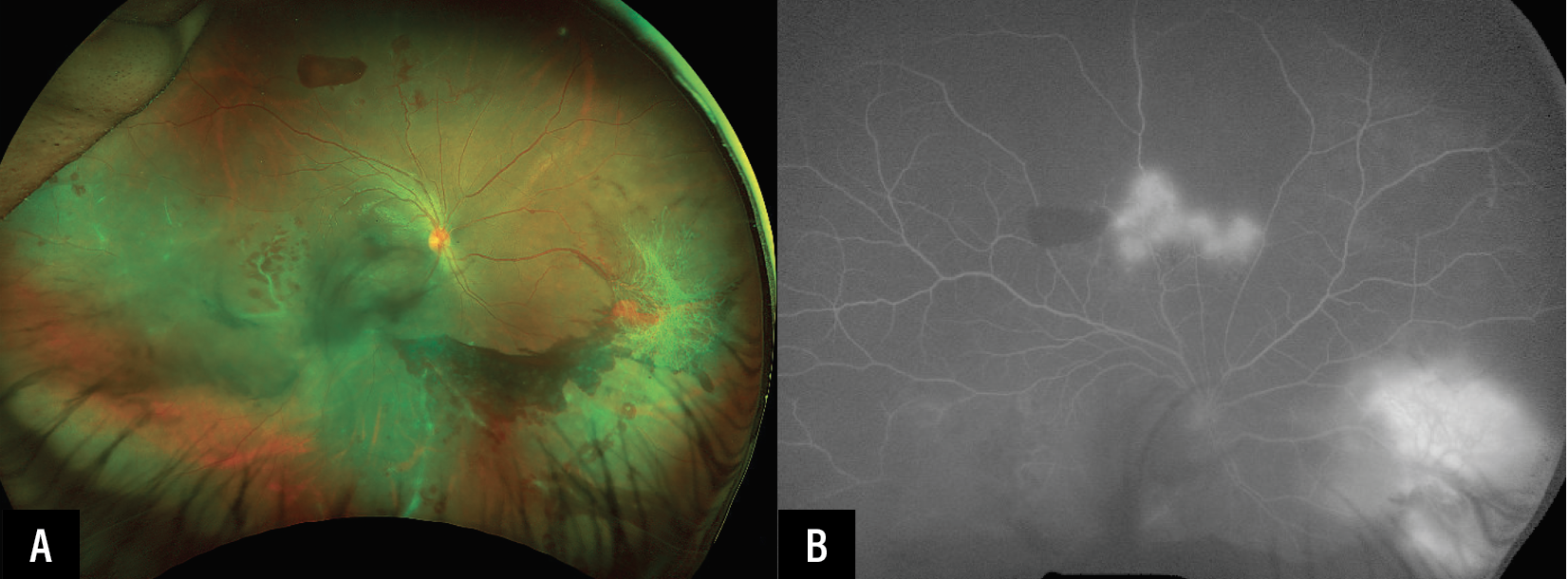 |
| Figures 9A-B. Idiopathic occlusive retinal vasculitis with superior peripheral capillary dropout, retinal neovascularization, vitreous hemorrhage and pre-retinal hemorrhage. |
Cases where uveitis referral may not be needed include mild, non-occlusive, and Zone 3 retinal vasculitis, especially post-vitrectomy without macular edema; well-controlled vasculitis associated with clear systemic diagnosis managed by a rheumatologist; and cases with a good response to a single administration of local corticosteroid agent or a typical oral corticosteroid taper without recurrence. However, even in mild cases, referral should be considered if there’s evidence of progression and/or visual decline.
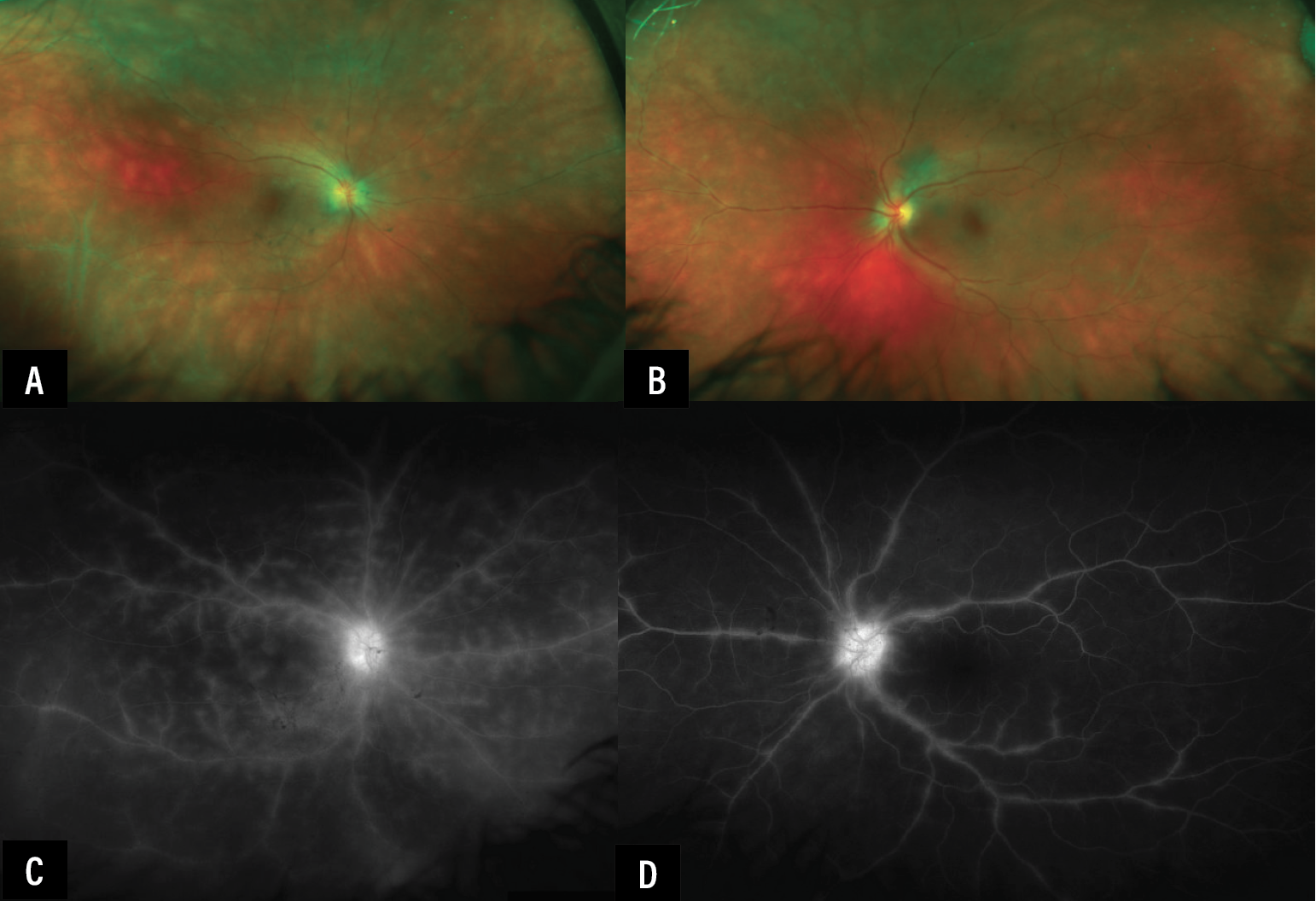 |
| Figures 10A-D. Large vessel phlebitis in a patient with birdshot choroidopathy. |
Conclusion
Retina specialists are often the first to diagnose retinal vasculitis. Once identified, evaluate for concomitant intraocular inflammation, rule out infectious and neoplastic masquerades, and assess the need for corticosteroids. In some circumstances, retina specialists may co-manage the structural and ischemic consequences, while the uveitis specialist helps control the inflammatory driver and assist in cases of diagnostic uncertainty and corticosteroid dependence needing consideration of IMT. Early collaboration can reduce delays in initiating appropriate systemic therapies and prevent irreversible vision loss. RS
REFERENCES
1. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol 2005;140:3:509–16.
2. Agarwal A, Rübsam A, Zur Bonsen L, Pichi F, Neri P, Pleyer U. A comprehensive update on retinal vasculitis: Etiologies, manifestations and treatments. J Clin Med 2022;11:9.
3. Arora A, Agarwal M, Loh NC, et al. Diagnostic workup of retinal vasculitis: An algorithmic approach. Ophthalmologica 2024;247:5-6:280–292.
4. Knickelbein JE, Tucker W, Kodati S, Akanda M, Sen HN. Non-invasive method of monitoring retinal vasculitis in patients with birdshot chorioretinopathy using optical coherence tomography. Br J Ophthalmol 2018;102:6:815–820.
5. Dhirachaikulpanich D, Chanthongdee K, Zheng Y, Beare NAV. A systematic review of OCT and OCT angiography in retinal vasculitis. J Ophthalmic Inflamm Infect 2023;13:1:1.
6. Birnbaum AD, Fawzi AA, Rademaker A, Goldstein DA. Correlation between clinical signs and optical coherence tomography with enhanced depth imaging findings in patients with birdshot chorioretinopathy. JAMA Ophthalmol 2014;132:8:929–35.
7. Noori J, Leal C, Ding K, Shah VA, Kingsley RM. Validity of spectral-domain optical coherence tomography angiography for detection of retinal vasculitis. Ophthalmic Surg Lasers Imaging Retina 2026:1–8.
8. Wu AL, Guo Y, Hao J, et al. Tubercular retinal vasculitis in widefield optical coherence tomography angiography. Am J Ophthalmol Case Rep 2026;41:102527.
9. Cifuentes-González C, Le Tong Y, Mejía-Salgado G, et al. Global demographic and etiological variations of retinal vasculitis: A systematic review and meta-analysis: International Uveitis Study Group (IUSG) Retinal Vasculitis Study (ReViSe) Report 1. Surv Ophthalmol 2025;70:4:756–770.
10. Thomas AS, Redd T, Campbell JP, et al. The impact and implication of peripheral vascular leakage on ultra-widefield fluorescein angiography in uveitis. Ocul Immunol Inflamm 2019;27:3:349–355.
11. Karaca I, Uludag G, Matsumiya W, et al. Six-month outcomes of infliximab and tocilizumab therapy in non-infectious retinal vasculitis. Eye (Lond) 2023;37:11:2197–2203.
12. El-Asrar AM, Al-Kharashi SA. Full panretinal photocoagulation and early vitrectomy improve prognosis of retinal vasculitis associated with tuberculoprotein hypersensitivity (Eales’ disease). Br J Ophthalmol 2002;86:11:1248–51.
13. Okinami S, Sunakawa M, Arai I, Iwaki M, Nihira M, Ogino N. Treatment of pars planitis with cryotherapy. Ophthalmologica 1991;202:4:180–6.



