Take-home points
|
 |
Bio Dr. Khan is a vitreoretinal surgeon in Granite Bay, Calif. |
Several surgical techniques combine pars plana vitrectomy and secondary intraocular lens placement, using the skillset and instrumentation of the vitreoretinal surgeon.1 In the past several years, two techniques have experienced considerable adoption: flanged intrascleral haptic fixation (FISHF) and Gore-Tex suture fixation.2,3 Several studies have published postoperative complication rates, with technique refinement and natural progression along surgical learning curves resulting in improving outcomes over time.4
The question remains: Which technique is “best?” As clinical outcomes have informed, both techniques can achieve excellent results.2-4 Ultimately, two factors remain critical for both physician and patient: refractive outcomes and stable IOL position. For this reason, sutured scleral fixation using Gore-Tex suture continues to serve as an excellent surgical option.
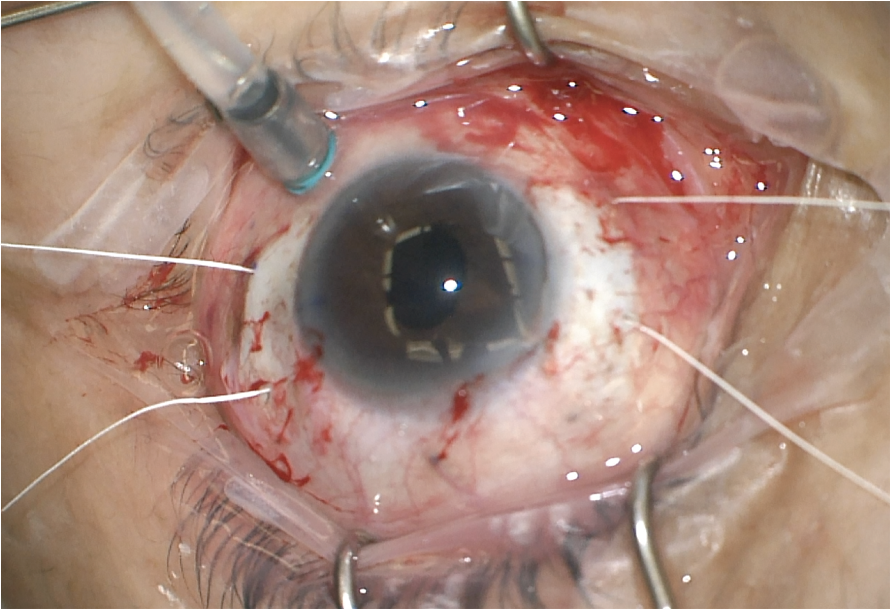 |
| Figure 1. True four-point fixation using Gore-Tex suture and an Akreos AO60 IOL results in a stable IOL position with reliable refractive outcomes. In-the-bag IOL calculations can be used when sclerotomies are placed 3 mm posterior to the limbus. |
Refractive Stability
Gore-Tex suture fixation allows for true or pseudo four-point fixation of an IOL (Bausch & Lomb Akreos AO60 and enVista MX60, respectively). This four-point fixation allows for stable IOL position and, therefore, refractive stability (Figure 1).
Several groups have reported favorable refractive outcomes using in-the-bag IOL calculations. A cohort study of 55 eyes reported refractive outcomes following scleral fixation of an Akreos AO60 (n=47) or enVista MX60 (n=8) IOL.5 Using in-the-bag calculations, mean deviation from refractive target aim was -0.43 ±0.71 D for fixation 3 mm posterior to the limbus at mean 9.7 months, with no significant difference between the Akreos A060 and the enVista MX60 respectively (-0.43 ±0.71 D and -0.36 ±1.02 D; p=0.82).5 Another study also noted excellent refractive outcomes using in-the-bag calculations, with an average prediction error (postoperative spherical equivalent refraction minus target refraction) at -0.19 ±0.72 D.6 In-the-bag calculations using Barrett II, SRK/T, Holladay 2 and Hoffer Q formulas were non-inferior to each other.6
| Read the counterpoint article here. |
These results were replicated by other studies. One group reported refractive outcomes in 27 eyes undergoing PPV and Gore-Tex suture fixation.7 Mean postoperative spherical equivalent refraction was -0.35 ±1.34 D at mean 200 days of follow-up. Across all eyes, 75 percent of eyes were within ±1 D of target refractive aim. Similarly, another study reported refractive outcomes in 63 eyes undergoing scleral fixation of an Akreos AO60 IOL.8 In the 63 eyes evaluated, mean final postoperative uncorrected visual acuity was 0.31 ±0.22 (20/41 Snellen equivalent). Mean postoperative spherical equivalent was
-0.57 D, with 63 percent of eyes within ±0.5 D of the refractive target.
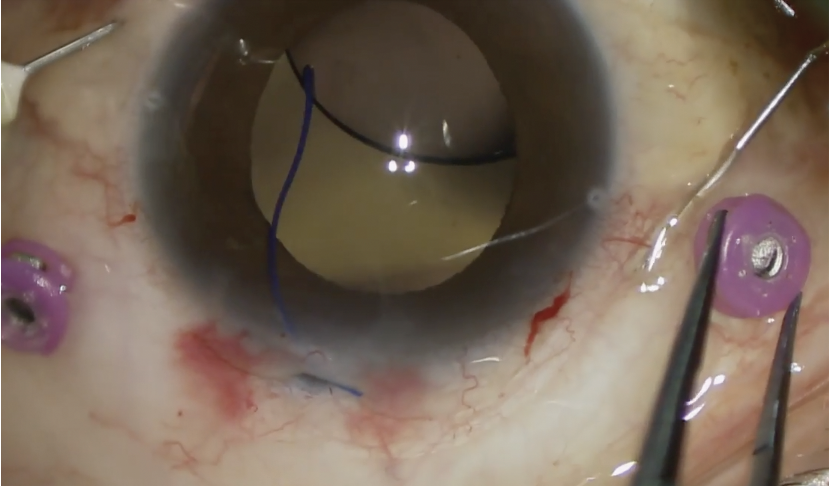 |
| Figure 2. When using the FISHF technique, care must be taken to avoid deformity of haptics. Stress on the haptic-optic junction may occur when haptics are passed through scleral passages, whether created with needles or trocar-cannulas. |
Avoiding IOL Tilt
In addition to refractive stability, four-point fixation helps avoid issues with postoperative IOL tilt or malposition.
When using FISHF, symmetry of scleral passages is critical to avoiding tilt, leading to the development of instruments to ensure symmetrical needle passes as best as possible.9 Several reports have also described haptic deformity or instability of the haptic-optic junction when using the FISHF technique (Figure 2), resulting in mild to severe IOL tilt. For instance, a study reported 18 cases of spontaneous, severe tilt following FISHF of a CT Lucia 602 (Carl Zeiss Meditec) IOL.10 Commonly referred to the “IOL rotisserie” phenomenon, authors noted free rotation of haptics within the optic insertion as the source of IOL tilt. Application of laser to the haptic-optic junction may mitigate this issue11—referred to as a “laser-lock”—but junction instability may still occur. Additional haptic related issues have also been reported. For example, researchers reported clinicopathological findings in 12 explanted CT Lucia 602 IOLs following FISHF. When analyzing the explanted haptics, the authors noted 15 were deformed, six were broken, two were detached and four exhibited free rotation within the optic insertion.12
Comparative studies have described differences in the rate of IOL tilt between FISHF and sutured approaches. In an analysis of 511 eyes undergoing IOL exchange surgery, FISHF was associated with a significantly greater frequency of IOL tilt (11.8 percent) compared to four-point suture fixation (1.1 percent, p= 0.01).13
Minding the Flange
A key consideration with FISHF is the stability of the haptics within the sclera over time. The adoption of flanged haptics helped reduce the risk of IOL dislocation from haptic slippage through scleral passages.14 However, cases of IOL dislocation may occur even despite flanged haptics, and flange exposure may occur as a late complication of the technique.
A meta-analysis of postoperative complications following ISHF compared complication profiles of ISHF using various methods, including scleral tunnels, glue assisted or flanged modifications.15 The authors noted operative time was shorter and best-corrected visual acuity was better when using the FISHF technique, but rates of haptic exposure (6.5 percent), iris capture (5.4 percent) and IOL dislocation (7.3 percent) were highest using the flanged technique.15 Moreover, a study of 488 eyes reported that IOL dislocation still occurred in 6.6 percent of eyes with flanged haptics, although these were primarily in cases where a previously placed IOL was repositioned.16
 |
| Figure 3. Care must be taken to ensure flanged haptics are deposited into the sclera to avoid later exposure. |
Flange exposure must also be monitored. In a series of FISHF eyes with a mean follow-up of 3.3 years, the flange exposure rate was 14 percent (21/150 flanges), and flange diameter was noted as a risk factor for exposure (OR 1.012, p=0.023).17 The authors noted conjunctival thinning in areas of flange exposure, introducing a possible pathway for endophthalmitis. While no such cases of endophthalmitis due to exposed flanges were reported in that study, two cases (0.4 percent) were noted in the 488-eye series described above.16 The authors noted the importance of confirming flanged haptic ends are deposited within the scleral tunnels (Figure 3), which may require haptic trimming to achieve.14,17
Conclusions
Several effective options exist for secondary IOL placement that fit well within the scope of the vitreoretinal surgeon. The FISHF technique is an excellent option, though issues with IOL tilt, haptic-optic junction instability and flange exposure are important considerations. Certainly, there are arguments against use of Gore-Tex or other suture-based techniques. These include suture-related concerns, such as suture exposure due to conjunctival erosion or suture breakage, or IOL-related concerns, such as eyelet fracture18 or opacification of hydrophilic acrylic IOL19 material. Ultimately, surgeons may choose what’s best in their own hands, and many such complications can be effectively avoided with careful surgical planning, technique and preoperative judgement. RS
REFERENCES
1. Wagoner MD, Cox TA, Ariyasu RG, Jacobs DS, Karp CL, American Academy of Ophthalmology. Intraocular lens implantation in the absence of capsular support: A report by the American Academy of Ophthalmology. Ophthalmology 2003;110:4:840-859.
2. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology 2017;124:8:1136-1142.
3. Khan MA, Samara WA, Gerstenblith AT, et al. Combined pars plana vitrectomy and scleral fixation of an intraocular lens using Gore-Tex suture: One-year outcomes. Retina 2018;38:7:1377-1384.
4. Mahmoudzadeh R, Oh GJ, Patel N, et al. Pars plana vitrectomy and scleral-fixated intraocular lenses: Comparison of Gore-Tex suture and flanged intrascleral haptic fixation techniques. Can J Ophthalmol 2025;60:1:e65-e72.
5. Su D, Stephens JD, Obeid A, et al. Refractive Outcomes after pars plana vitrectomy and scleral fixated intraocular lens with Gore-Tex suture. Ophthalmol Retina 2019;3:7:548-552.
6. Botsford BW, Williams AM, Conner IP, Martel JN, Eller AW. Scleral fixation of intraocular lenses with Gore-Tex suture: Refractive outcomes and comparison of lens power formulas. Ophthalmol Retina 2019;3:6:468-472.
7. Day HR, Durrani AK, Kim SJ, Patel S. Outcomes and complications of concurrent pars plana vitrectomy and scleral-fixated intraocular lens placement using Gore-Tex suture. J Vitreoretin Dis 2020;4:2:119-124.
8. Patel NA, Fan KC, Yannuzzi NA, et al. Refractive outcomes of four-point scleral fixation of Akreos AO60 intraocular lens using Gore-Tex suture. Clin Ophthalmol 2020;14:4431-4437.
9. Yamane S, Maruyama-Inoue M, Kadonosono K. Needle stabilizer for flanged intraocular lens fixation. Retina 2019;39:4:801.
10. Enright JM, Purt B, Bruck B, et al. Severe spontaneous tilt of scleral-fixated intraocular lenses. Am J Ophthalmol 2024;262:206-212.
11. Liu JC, Sheybani A. Haptic curing with endolaser after lens tilt in the Yamane technique. Am J Ophthalmol Case Rep 2024;34:102049.
12. Kelkar N, Eid K, Nakatsuka AS, Johnson C, Mamalis N, Werner L. Severe intraocular lens tilt after the Yamane technique. J Cataract Refract Surg 2025;51:2:126-132.
13. Patel V, Pakravan P, Lai J, et al. Intraocular lens exchange: Indications, comparative outcomes by technique, and complications. Clin Ophthalmol 2023;17:941-951.
14. Yamane S, Ito A. Flanged fixation: Yamane technique and its application. Curr Opin Ophthalmol 2021;32:1:19-24.
15. Nagino K, Inomata T, Ohta T, et al. Postoperative complications of intrascleral intraocular lens fixation: A systematic review and meta-analysis. Surv Ophthalmol 2025;70:3:489-498.
16. Patel KG, Yazdani A, Abbey AM. Twenty-five and twenty-seven-gauge sutureless intrascleral fixation of intraocular lenses: Clinical outcomes and comparative effectiveness of haptic flanging in a large single-surgeon series of 488 eyes. Retina 2021;41:12:2485-2490.
17. Xu F, Jiang H, Mu J, et al. Long-term clinical outcomes of a modified Yamane technique for intrascleral sutureless posterior chamber intraocular lens fixation. Am J Ophthalmol 2026;282:187-196.
18. Watane A, Botsford BW, Sood AB, et al. Scleral-sutured intraocular lens dislocations secondary to eyelet fractures. Am J Ophthalmol 2021;221:273-278.
19. Belin PJ, Kim JH, Sheikh A, Winokur J, Rhee D, Deramo V. Incidence and risk of scleral-fixated Akreos (AO60) lens opacification: A case series. J Vitreoretin Dis 2021;5:2:157-162.



